


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Vascular Variability in Anterolateral Thigh Flap According to Arteriography in the Mexican Population
Imelda Diaz Ruiz1, Josafat Yair Arroyo Aparicio2, Mauro Gerardo Vazquez Armenta3, Brenda Valdez Diaz4, Daniel Flores Rodriguez5, Carlos Eduardo Rodriguez Rodriguez6, Pedro Leonardo Villanueva Solorzano6, Alberto Robles Mendez Hernandez6, Luis Angel Medina Andrade7, Alejandra Lizbeth Salinas Atriano7
2.Orthopedic Surgery Resident, Postgraduate School in Naval Health, Centro Medico Naval, Universidad Naval, Mexico.
3.Plastic, Aesthetic and Reconstructive Surgery, Microsurgery, Centro Medico Naval, Mexico City, Mexico.
4.General Surgery Service Resident, Centro Medico Nacional Siglo XXI, Mexico City. Mexico.
5.Plastic, Aesthetic and Reconstructive Surgery, Centro Medico Nacional 20 de noviembre ISSSTE, Mexico City, Mexico.
6.General Surgery Resident, Universidad La Salle, Hospital Angeles Metropolitano, Mexico City, Mexico.
7.General Surgeon, Medical Student*, Hospital General de Zona #30 IMSS, Mexico City, Mexico.
Copyright :© 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Objective: To determine the vascular variability in Mexican population submitted to anterolateral thigh flap.
Material and Methods: We performed a retrospective, transversal analysis of patients submitted to medial thigh lift in the Hospital General de Mexico during the period from 2013 to 2016. Of a total of 95 patients with this procedure, only 45 complete the inclusion criteria and were analyzed in their clinical and arteriography characteristics, with posterior statistical analysis with Stata 11.1 software.
Results: Of the 95 patients with medial thigh lift, 40 were excluded. Of the remaining 45 patients, 35 were males and 10 females. The statistical analysis found that perforating A type was the most common in females, while B was the most common in males according to the classification of Yu. Other analyzed variables include the length of the perforating vessels, with type A of 21.85mm, perforating B of 25.27mm and the perforating C of 34.8mm; and the diameter of perforating A of 2.84mm, B of 2.46mm and C of 2.15mm.
Conclusions: with this advanced comprehensive anatomy of the vascularity in the anterolateral thigh region we showed that is possible to increase the length and diameter of the incision of the anterolateral thigh lift with no significant increase in risk; specially with perforating type A, that is more common in females, as this procedure continues being the most popular and used due to its functional and cosmetic results.
Anterolateral Thigh Flap, Vascular Variability, Flap Viability, Arteriography ,Surgery
1. Introduction
Since the introduction by Song and colleagues in 1984, the anterolateral thigh flap was described for head and neck scars in patients with burns1, it has become popular and very accepted by their versatility, ideal for numerous reconstructions, with minimal morbidity in the donor site[1,2].
The anterolateral thigh flap could be designed as myocutaneous ( including the rectus femoral, the vastus lateral or the tensor of the fascia lata), fasciocutaneous, adipofascial or inclusive suprafascial.[3] It could be a simple or mixed flap, their dissection allows us to create a free or pediculate flap, or inclusive a neurocutaneous flap including the femoral lateral cutaneous nerve[3,4].
Between the benefits of this flap are their length of 4-35cm with a median of 16cm, width of 4-25 cm with a median of 8cm, thickness of 0.5 - 2.8 cm with a median of 0.64cm, the extension of body surface is between 70 – 240cm2 (with a median extension of 140cm2 and the primary closure of this flap could be achieved when the defect is between 7 – 9 cm.[5]
After a systematic review of the literature, the indications for the use of this flap is very wide, including head and neck reconstructions, procedures in the thorax, abdominal wall, breast, thoracic member and pelvic member[6].
The vascular anatomy of the anterolateral thigh flap depended on a septocutaneous perforating artery, as described initially, but Koshima found this characteristic in 5 of 13 patients and Xu described that cutaneous perforating vessels can be classified in two types, the 59.8% of musculocutaneous type crossing the vastus lateral muscle, and the 40.2% septocutaneous, passing across the muscular septum between the vastus lateral and rectus femoral. However, the vascular anatomy is not as consistent as Song suggests, and many other anatomical variations have been reported about the perforating arteries origin[7,8]
The femoral circumflex artery arises from the Deep femoral, although 10-25% of the cases from the common femoral and the iliac artery in 6%.[9]
The branches of the circumflex femoral and lateral artery include the ascending, descending, transverse and oblique. The descending branch could arise from the deep femoral (17,1 %) and common femoral ( 1,4 %).[10]
The initial description of the oblique branch of the lateral circumflex femoral artery was described by Wong, mentioning the presence in 35% of the patients[11]. The origin of the oblique branch is very variable, with the next variations: of the descending branch 35.5%-85.7%, the transversal branch 51.6%, from the femoral lateral circumflex artery 6.5%, from the Deep femoral in 3.2%, and from the common femoral artery in 3.2%.
The perforating arteries that irrigate the anterolateral thigh flap come from the descendent branch of the femoral circumflex artery in 57 to 100% of the patients[12], the perforating from the ascendant branch are reported in 2.6 to 14.5% of the cases, from the transversal branch in 4-25% of patients, perforating from the oblique branch in 14-43%, from the femoral circumflex in 1 - 12,9%, from the deep femoral in 1.4 to 11%, and from the common femoral in 1.4-1-8% of the cases[9,13,14].
The international literature reports that the incidence of absence of perforating branches is about 0.89 to 5.4%[6,7].
The perforating branch of the descendent branch of the femoral circumflex lateral artery is identified to dissect until the intermuscular septum between the vastus lateral and rectus femoral, the dissection is suffered from distal to proximal, and the lateral vessel is separated from the rectus lateralis, identifying the descendent branch of the femoral circumflex lateral artery and their perforating branches[6,7].
Saint - Cyr draws a line from the anterosuperior iliac spine to the superolateral border of the knee tag that corresponds with the intermuscular septum. A second line is drawn from the medial point of the initial vertical line to the medial point between the anterosuperior iliac spine and the symphysis of the pubis. This second line corresponds with the descendent branch of the femoral circumflex lateral artery (Figure. 1). Saint – Cyr describes that the more frequent perforating branches are identified in the medial point, according to the Yu system, described posteriorly and that corresponds with the point B.[15,16]
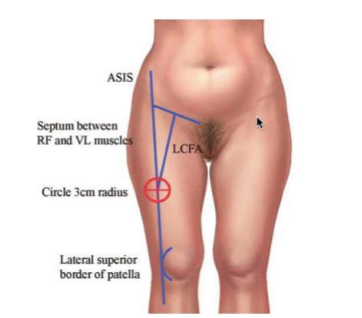
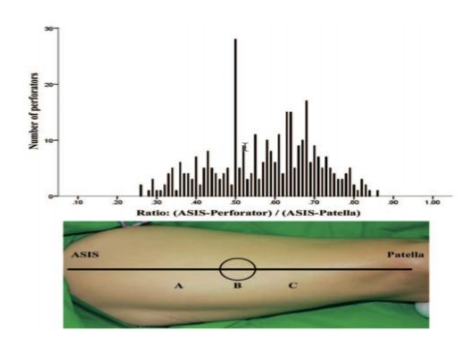
In a systematic revision from 1948- 2012 by Michael Saint- Cyr, the total of perforating vessels was in relation with the medial point of marked area, with a diameter of about 3-6cm, with more perforating vessels in the inferolateral area of the circle, with a percentage of 47- 95 % and the perforating vessels that were 5cm proximal to the medial point are 51% and 5cm distal 49% of the patients[7].
Xu and cols. reported that 92% of the perforating vessels are located in a circle of 3cm around the mentioned area[17].
Zhou found that the point of exit of the perforating vessel was located in the intermuscular septum, lateral to the lateral vastus and generally this is 2cm lateral and inferior to the medial point of the line that connects the anterosuperior iliac spine and the superolateral border of the knee tag[18].
Kimata and cols confirmed that the perforating vessels were concentrated in the medial point of the line that bond the anterosuperior iliac spine and the superolateral border of the knee tag[19].
Actually, about 50 different flaps have been described, some of them that could be transferred in a free form or by microsurgery. In our team we have the experience with the anterolateral thigh flap, offering a well-vascularized flap, healthy, with a size from 35- 40 cm, that allow us to reconstruct bloody areas destined for amputation, incapacity, and immobility, offering low complications or aftermath in the donor area too.
In the Hospital General de Mexico as in other many centers that use flaps with microsurgery, the more frequent flap used is the anterolateral thigh flap by the good results. In our center, an arteriography is performed previously for the procedure to determine the viability of the vessels, the diameter, size, number of perforating vessels and which could offer us the better results.
There no exist in the Mexican population studies that determine the frequency of anatomical variants of the perforating vessels of the lateral femoral circumflex descendent, however, with the registry by Doppler of the anatomy of this vessels is possible to determine the anatomic variants that are more common in the studied population; knowing that frequency allow us to compare if there is association between some variables like age or sex, and with that information complete a presurgical evaluation considering those factors to avoid or reduce the risk of failure, especially in centers when could be impossible to perform advanced imaging studies.
2. Material And Methods
This was an observational, retrospective, transversal study, developed in the Plastic and Reconstructive Surgery Service together with the Interventional Radiology of the Hospital General de Mexico. A preformed instrument for data recollection was created. We analyzed the files of all the patients that underwent arteriography previous to a microsurgical flap from January 2013 to January 2016.
The inclusion criteria were that the patients were a candidate to microsurgical treatment with anterolateral thigh flap, have a complete clinical and radiological file with arteriography of lower limbs, from 1 to 80 years old, any gender.
A review of 95 arteriographies was performed, 40 of those were not included in the study secondary to the bad definition in the study, without identification of perforating vessels or significant data were not recorded, in some of the studies the patients presented hypertension and the study was suspended.
At the end 45 arteriography’s were included, 35 males and 10 females, with an adequate definition of perforating vessels of the lateral circumflex femoral descending artery, with the report of length and diameter of those perforating vessels according to the Yu classification.
3. Results
The statistical analysis was performed with medial tendency measures using the statistical software Stata 11.1, Corp 4905. From the total of 90 patients, 45 complete the inclusion criteria, 35 were male and 10 females.
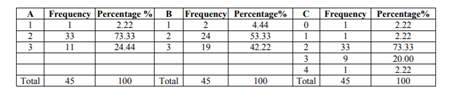
According to the statistical analysis, the most frequent perforating vessel in females was type A, according to Yu classification (table 1), with a mean of 2.4. In the male sex, the most frequent perforating vessel was type B (mean 2.4, table 2). The most frequent perforating vessel in all the population was the perforating B (Table 3). The population presented a mean of 2 perforating vessels in each patient, however, we found that the greatest variability was with the perforating type C, identifying a patient without perforating vessels and one patient with four of them (Table 4).



The factors included in the statistical analysis were the length of the perforating vessels, with an average of 21.85mm in the type A in females, type B 25.27mm and type C 34.8mm, identifying the type A with shorter length 6.4mm and greater length in type C with 77.2mm (Table 5); In the male sex the average of type A was 31.3mm, type B 26.1mm and type C 32.4mm, the shorter length was 2.1mm corresponding to the type A but the greater length was type A too, with 74.2mm (Table 6). From the total study population the average perforating vessel type A length was 29mm, type B 25.9mm and type C 32.9mm, with the shorter perorating vessel corresponding to type A (2.1mm) and the greater type C (77.2mm)(Table 7).



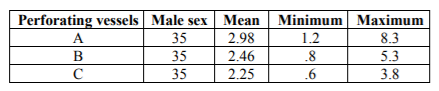
Some of the measures identified in the vascular variants from the perforating vessels according to Yu classification were the diameter of the vessel, after the analysis we found that male sex (Table 8) had a diameter of perforating vessels type B (0.8mm) and C (0.6mm) was of smaller caliber compared with females (Table 9), reported in 1.3 mm (B) and 0.89mm respectively; The average of perforating vessels diameter was 2.84mm for type A, 2.46mm for type B, and 2.15mm for type C. (Table 10).


4. Discussion
The development of microsurgical techniques has increased the horizons of traditional plastic and reconstructive surgery, and being considered actually one of the main resources of modern reconstructive surgery. In developed countries the use of microsurgical techniques is a routine and the first option as a solution of problems in the head and neck, thorax, abdomen, and extremities, where the reconstructive options were running out, bordering on taking measures such as the amputation of some limbo r the inability of an anatomical area.
In the Hospital General de Mexico, the plastic and reconstructive surgery service give consult to 7 to 10 patients per month that need a microsurgical reconstruction in areas like head, neck, thorax, abdomen or extremities, and the most frequent technique used in those patients is the anterolateral thigh flap. Those patients are submitted to a microsurgical protocol to decide the best reconstructive option. The literature mention that some vascular variables exist in relation to the perforating vessels of the mentioned flap, for this reason in our unit a presurgical arteriography is performed, to evaluate the blood flow of a certain blood vessel and identify anatomical aspects like vascular variations that could influence the viability of the flap.
In 2004 Yu describes the ABC system to elucidate the distribution and location of the perforating vessels. In that study Yu and cols. identified one to three cutaneous perforating vessels in the anterolateral thigh flap, and named those A, B, and C, from proximal to distal. Type B is found near the medial point of a line that connects the anterosuperior iliac spine and the superolateral border of the knee tag. The type A and C are located 5cm proximal and distal to B type, respectively[20].
When the perforating vessels were categorized in the system ABC of Yu, the ones in the proximal A point were identified in 42.7% of the patients, the perforating vessels in point B in 80% of the patients, and the ones in the point C were identified in 87.3% of the patients. The perforating vessels in the point C represent 51,4% of the patients, in the B point the 31,9 %, and in the A point the 16,7%. According to the study by Yaou-Chao Lee in 2014, Taiwan, using the Yu classification, the mean distance between the anterosuperior iliac spine and the skin location of the perforating vessel was 15,3 ± 2,8 cm for the A point, 21,1 ± 2,6 cm for the B point, and 28,4 ± 3,4 cm for the C point[8,20].
The most unfavorable aspect of the anterolateral thigh flap is their complex vascularity in occidental population compared with the Asian populations, with similarities in A and B, but not C. Yaou Chao Lee founds that the C perforator was more frequent (87,3%). Saint-Cyr and cols. proposed an algorithm for the selection of perforating vessels in B point that is used frequently reporting between 57 to 100 % of perforating vessels. This difference could be attributed to the high size of the patients (20cm vs 15cm) or gender, and for this reason is an ideal flap for reconstruction, our research was to identify the most frequent perforating vessel for the use of this flap in Mexican population by arteriography. [21-23]
Before the flap dissection, some aspects must be considered like locations and number of perforating vessels, type of perforating vessel (septocutaneous or muscle-cutaneous), flap pedicle (ascendant branch, oblique, transversal or other), and length and diameter of the vessels.
In the Mexican population, we found after arteriography that the most frequent perforating vessel is the B, with the longest perforating vessel being the type C, and the one with the better diameter the type A. (See table 3,7,10)
In the worldwide literature is reported that the length of perforating vessels in this area is 1.5mm to 60.2mm (average of 38.8mm) and in the Mexican population is 2.1mm to 77.2mm (average 32.9mm); the perforating vessels diameter of descendent artery is 1,3 mm (range 0.9- 10.8 mm), and in our population with a mean of 2.46 mm (range 0.6mm- 8.3mm)[25,26].
5. Conclusions
With this advanced comprehension of the vascular anatomy of the anterolateral thigh region by arteriography, the dissection of an anterolateral thigh flap could be performed in a secure manner and continue being the most frequent flap used for a minimal loss of function and a donor site cosmetically acceptable.
The selection of perforating vessels requires clinical and surgical experience by the surgeon, but can be more easy with the help of imaging studies like arteriography describing the diameter, length and location of the perforating vessels, to select the better option and perform a free or pedunculated flap with the certain of the excellent blood flow without flap compromise.
References
- Song YG, Chen GZ, Song YL. The free thigh flap: a new free flap concept based on the septocutaneous artery. Br J Plast Surg 1984;37:149-59.
- Song R, Song Y, Yu Y, et al. The upper arm free flap. Clin Plast Surg 1982;9:27-35.
- WeiFC,JainV,CelikN,ChenHC,ChuangDC,LinCH .Have we found an ideal soft-tissue flap? An experience with 672 anterolateral thigh flaps. Plast Reconstr Surg. 2002;109:2219– 2226.
- Hanasono MM, Skoracki RJ, Silva AK, Yu P. Adipofascial perforator flaps for “aesthetic” head and neck reconstruction. Head Neck 2011;33:1513–1519.
- Tommaso Agostini, Giulia Lo Russo, Yi Xin Zhang, Giuseppe Spinelli, Davide Lazzeri. Adipofascial Anterolateral Thigh Flap Safety: Applications and Complications, APS 2013; 40: 92-96.
- Michel Saint-Cyr, M.D. Georgette Oni, M.D. Michael Lee, M.D. Christina Yi. Simple Approach to Harvest of the Anterolateral Thigh Flap, Plast Reconstr Surg. 2012;129:207– 212.
- Chrisovalantis Lakhiani, Michael R. Lee, Michel Saint-Cyr. Vascular Anatomy of the Anterolateral Thigh Flap: A Systematic Review Plast. Reconstr. Surg. 2012; 130: 1254- 1268.
- Yao-Chou Lee, Wei-Chen Chen, Ting-Mao Chou, Shyh-Jou Shieh. Anatomical Variability of the Anterolateral Thigh Flap Perforators: Vascular Anatomy and Its Clinical Implications Plast. Reconstr. Surg. 2015;135: 1097 - 1107.
- Kimata Y, Uchiyama K, Ebihara S, Nakatsuka T, Harii K. Anatomic variations and technical problems of the anterolateral thigh flap: A report of 74 cases. Plast Reconstr Surg. 1998;102:1517– 1523
- Wong CH, Wei FC, Fu B, Chen YA, Lin JY. Alternative vascular pedicle of the anterolateral thigh flap: The oblique branch of the lateral circumflex femoral artery. Plast Reconstr Surg. 2009;123:571–577.
- Wong CH, Ong YS, Wei FC. The anterolateral thigh–vastus lateralis conjoint flap for complex defects of the lower limb. J Plast Reconstr Aesthet Surg. 2012;65:235–239.
- KekatpureVD,TrivediNP,ShetkarG,et al. Singleper forator based anterolateral thigh flap for reconstruction of large composite defects of the oral cavity. Oral Oncol. 2011;47:517–521.
- Wolff KD, Kesting M, Thurman ller̈ P, Bockmann R, Ho lzlë F. The anterolateral thigh as a universal donor site for soft tissue reconstruction in maxillofacial surgery. J Craniomaxillofac Surg. 2006;34:323–331.
- Seth R, Manz RM, Dahan IJ, et al. Comprehensive analysis of the anterolateral thigh flap vascular anatomy. Arch Facial Plast Surg. 2011;13:347– 354
- Michel Saint-Cyr, Georgette Oni, Michael Lee. Simple Approach to Harvest of the Anterolateral Thigh Flap, Plast. Reconstr. Surg.2012; 129: 207-211
- Yu P. Characteristics of the anterolateral thigh flap in a Western population and its application in head and neck reconstruction. Head Neck 2004;26:759– 769.
- Xu DC, Zhong SZ, Kong JM, et al. Applied anatomy of the anterolateral femoral flap. Plast Reconstr Surg. 1988;82:305–310.
- Zhou G, Qiao Q, Chen GY, Ling YC, Swift R. Clinical experience and surgical anatomy of 32 free anterolateral thigh flap transplantations. Br J Plast Surg. 1991;44:91–96.
- Kimata Y, Uchiyama K, Ebihara S, Nakatsuka T, Harii K. Anatomic variations and technical problems of the anterolateral thigh flap: A report of 74 cases. Plast Reconstr Surg. 1998;102:1517– 1523.
- Yu P. Characteristics of the anterolateral thigh flap in a Western population and its application in head and neck reconstruction. Head Neck 2004;26:759– 769.
- Shieh SJ, Chiu HY, Yu JC, Pan SC, Tsai ST, Shen CL. Free anterolateral thigh flap for reconstruction of head and neck defects following cancer ablation. Plast Reconstr Surg. 2000;105:2349–2357; discussion 2358
- Kimata Y, Uchiyama K, Ebihara S, et al. Anterolateral thigh flap donor-site complications and morbidity. Plast Reconstr Surg. 2000;106:584–589.
- Koshima I, Nanba Y, Tsutsui T, Takahashi Y. New anterolateral thigh perforator flap with a short pedicle for reconstruction of defects in the upper extremities. Ann Plast Surg. 2003;51:30–36
- Sananpanich K, Tu YK, Kraisarin J, et al. Flow-through anterolateral thigh flap for simultaneous soft tissue and long vascular gap reconstruction in extremity injuries: anatomical study and case report. Injury. 2008;39: S47YS54
- Xiao-Qing He, MD,*Þ Yue-Liang Zhu, MD, Þ Yi Wang, MM, Þ Liang-Bin Mei, MM, The Role of the Distal Runoff Vessel of the Descending Branch of the Lateral Circumflex Femoral System in Anterolateral Thigh Flap Surgery, Ann Plast Surg. 2016;77:73–79.