


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
The Prevalence of Food Insecurity among Pregnant Women participating in a Community-based Intervention Program
Nweze Nnakwe*, PhD, RDN, LDN
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: Food insecurity is practically a new approach and a more indicative measure of malnutrition. In Nigeria, despite various interventions in the past decades, malnutrition continues to be a serious public health problem and a contributing factor to high incidence of maternal and infant mortality. However, research studies on the frequency of food security in pregnant women especially in rural communities is limited. The purpose of this study was to determine the prevalence of food insecurity and factors that may contribute to food insecurity among pregnant women who participated in a community-based intervention program.
Methods: Four hundred and forty-nine pregnant women were recruited after they had enrolled in a community-based prenatal intervention program. The participants gave oral consent to be in the study and received a note containing the name of trained nurses to contact for debriefing. Data were collected for three years from participants who volunteered, using confidential questionnaire containing demographic characteristics. The participants also responded to a six-question subscale out of the 18 question Food Security Module, developed by the United States Department of Agriculture (USDA). Data was statistically analyzed using SPSS computer software. Pearson Chi-square was used to evaluate the differences between food insecurity levels and multivariate regression analysis was used to determine the contributing factors to food insecurity.
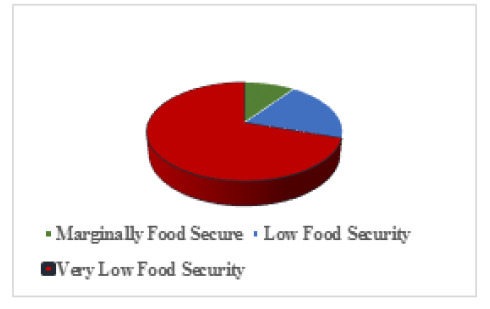
Results: Ten percent of the respondent were marginally food secure, 20% were low food secure and 70% were classified as very low food security at p< 0.05. The participants with less than school education was significantly food insecure at p< 0.001.
Food insecurity, age, education levels, and number of children.
1. Introduction
Food security occurs when all people, at all times, have physical, social, and economic access to sufficient, safe, and nutritious food that meets their dietary needs and food preferences for an active and healthy life [1]. Food insecurity is the opposite of food security. It is defined as lack of access to enough food to meet basic needs, including limitations in the quality, quantity, and/or frequency of food intake [2-4].Food insecurity exists whenever the availability of nutritionally adequate and safe foods or the ability to acquire acceptable foods in socially acceptable ways is limited or uncertain [5]. Four main conceptual elements define this phenomenon [6]: First, food insecurity is experienced at the household and individual levels in different ways. Individual-level experience relates to issues of food consumption and allocation and includes the physiological sensation of hunger. Food supply management and acquisition issues define the household situation [7]. Second, the experience of food insecurity is not static but dynamic in nature, defined by a sequence of events and experiences that can be considered in terms of frequency, duration, and periodicity. Third, the sequence of stages that define the experience reflects graded levels of severity, ranging from qualitative compromises in food selection and consumption to quantitative compromises in intake and the physical sensation of hunger, as resources become depleted. At its most severe stage, food insecurity is experienced as absolute food deprivation (i.e., individuals not eating at all). Fourth, within households, individuals’ experiences of food insecurity differ. Mainly, adults seem to compromise their own intakes first, to minimize the extent and nature of compromise experienced by children in the household. This suggests that food insecurity is a managed process in which the sequence of events and severity of experience for different household members is, to some extent, controlled and predictable [8, 9].
Food insecurity is often linked to poverty, and malnutrition. Malnutrition affects a large proportion of pregnant women in many developing countries but has received minimum attention as an important determinant of poor maternal outcomes, intrauterine growth restriction, preterm birth, anemia, low birth weight, gestational diabetes and maternal and infant morbidity and mortality [10-12]. Malnutrition starts by consuming diets that are inadequate in essential nutrients such as protein, carbohydrates, fat, vitamins, and minerals. Insufficient consumption of nutrients causes under nutrition. Under nutrition during pregnancy or infancy can result in permanent problems with physical and mental development [13].
Laraia et al [14] suggested three possible reasons why food insecurity might have specific importance for women during pregnancy especially in developing countries: high nutrient demands, the effort required for food preparation may be more difficult, and pregnant women may be obliged to leave the workforce, especially in later pregnancy, which leads to financial pressure.
The world crisis of high food prices affects access to nutritious food. Low-income households do not have enough income to purchase foods. However, food choices are very sensitive to price, and dietary variety, including high essential nutrient foods. Foods high in important nutrients are the first to be excluded from the diet, as these options are usually more expensive. The food crisis is thus a dual threat to the quality and quantity of the diet, resulting in malnutrition. Women are especially vulnerable, with an increased risk of malnutrition during pregnancy [15].Hungry and sickly mothers bear malnourished and sickly infants. The purpose of this study was to determine the prevalence of food insecurity and factors that can contribute to food insecurity among pregnant women who participated in a community-based intervention program.
2. Methods and Procedures
Four hundred and forty-nine pregnant women were recruited after they had enrolled in a community-based prenatal intervention program. The participants gave oral consent to be in the study and received a note containing the name of trained nurses to contact for debriefing. Data were collected for three years from participants who volunteered, using confidential questionnaire containing demographic characteristics. The participants also responded to a six-question subscale of the 18 question Food Security Module, developed by the USDA. The subscale addressed the following areas: (1) not having enough money to buy food for a balanced meal (3 to 4 times a day), (2) adults cutting the size or skipping meals, (3) worried that food would finish before getting money to buy food, (4) adults not eating for a whole day, and (5) how often this happened.
Data from each questionnaire were coded and statistical analyses were conducted using the Predictive Analysis Software for Windows (PAWS Statistics, version 18.0; SPSS Inc., Chicago, IL). Multivariate regression analysis was used to determine the relationship between education level, number of children in the household, age and food insecurity. Pearson’s Chi-square test was utilized to evaluate the differences between food insecurity levels. Statistical significance was set at p< 0.05 level.
3. Results
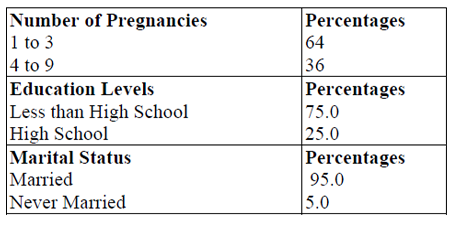
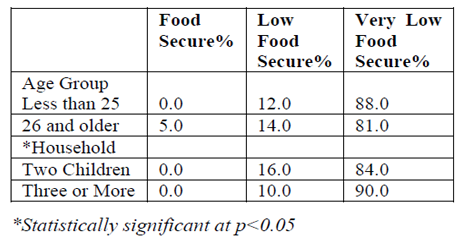
Figure 1 shows that 10 percent of the respondents were marginally food secure, 20 % experienced low food security and 70% were classified as very low food security; the differences were statistically significant at p< 0.05. The participants with less than high school education were significantly food insecure than those with high school or higher at p< 0.001. In addition, participants with four or more children experienced more food insecurity than those with one to three children. This was statistically significant at p< 0.05. In Table 1 shows that 75.0 percent had less than high school education, and 95 percent were married. In Table 2, 88% of participants ages 25 years or less had very low food security while 81% of those 26 years old or less had very low food security. In addition, participants with three or more children experienced more food insecurity than those with one of two children. The difference was statistically significant at p< 0.05.
4. Discussions
This study aimed to assess the prevalence of food insecurity among pregnant women in rural communities in Nigeria. Results show that majority of the participants were food insecure. Similarly, a population-based postpartum survey from California reported food insecurity in low income pregnant women[16]. In addition, a prospective cohort study of 810 pregnant low-income women in the United States showed 14% to be marginally food secure and 10% to be food-insecure households [6].
Results from this study also showed that educational status and the number of children in the household, and age were significantly associated with food insecurity. This finding is consistent with a study in rural communities in Malaysia, food-insecure women had less education, lower household income, and a greater number of children [17].Finally, in Nigeria, maternal and infant mortality is a common occurrence and a huge public health issue [18]. However, adequate prenatal care has been shown to reduce both maternal and infant morbidity and mortality. More maternal resources and education are needed in reducing food insecurity. It is important to note that younger pregnant women reported more food insecurity than the older participants. More studies are needed to determine the reasons for food insecurity among younger pregnant women.
5. Conclusion
Food insecurity is prevalent among pregnant women in the rural communities; and some of the contributing factors are level of education, the number of children in the household, and age. Adequate nutrient intake is essential during pregnancy, because well-nourished and healthy mothers deliver health babies.
6.References
- Life Sciences Research Office, F.o.A.S.f.E.B., Core indicators of nutritional state for difficulty-sample populations. J Nutr 1990. 120(suppl): p. 1559-1600.
- Tarasuk, V., Household food insecurity with hunger is associated with women's food intakes, health and household circumstances. J Nurtr., 2001. 131: p. 2670-2676.
- Bhattacharya, J., Currie, J., Haider, S. , Poverty, food insecurity, and nutritionalboutcomes in children and adults. . J Health Econ. , 2004. 23: p. 839–62.
- Kaiser, L.L., Melgar-Quinonez, H., Townsend, M.S., Nicholson, Y., Fujii, M.L., Martin, A.C., Lamp, C.L., Food insecurity and food supplies in Latino households with young children. . J Nutr Educ Behav. , 2003. 35: p. 148–53.
- Campbell, C.C., Desjardins, E. A., model and research approach for studying the management of limited food resources by low income families. J Nutr Educ., 1989. 21(4): p. 162–171.
- Radimer, K., Olson, CM., Greene, JC., Campbell, CC., Habicht, JP., Understanding hunger and developing indicators to assess it in women and children. J Nutr Educ., 1992. 24(1):p. 36S–45S.
- Radimer, K.L., Olson, C.M., Campbell, C.C.. Development of indicators to assess hunger. J Nutr, 1990. 120: p. 1544-8.
- Furness, B.W., Simon, S.P., Wold, C.M., Asarian-Anderson,J., Prevalence and predictors of food insecurity among low-income households in Los Angeles County. Public Health Nutrition, 2004. 7: p. 791-794.
- Nord, M., Andrews, M., Winicki, J., Frequency and Duration of Food Insecurity and Hunger in US Households. Journal of Nutrition Education and Behavior., 2002. 34(4): p. 194–201.
- Olawale, E.O., et.al, Between rainfall and food poverty: Assessing vulnerability to climate change in an agricultural economy. J of cleaner production, 2018. 98: p. 1-10.
- Wasiu, O., and Burhan, Ö., Comprehensive Review of Growing Food Insecurity in Africa in Terms of Causes, Effects and Solutions: The Nigerian Example. Turkish Journal of Agriculture: Food Science and Technology, 2017. 5(6): p. 629-636
- Dodi, W., An Exploration of Food Insecurity, Poverty, Livelihood and Local Food Potentials in Kulon Progo Regency, Indonesia. Forum Geografi, 2018. 32(1): p. 2460-3945.
- Holger, W.U., et. al., Undernutrition and malaria in pregnancy a dangerous dyad? BMC Medicine 2016. 14(142): p. 3-9.
- Laraia, B.A., Siega-Riz, A.M., Gundersen, C., Dole N., Psychosocial factors and socioeconomic indicators are associated with household food insecurity among pregnant women. J Nutr., 2006. 136: p. 177–182.
- World Health Organization, Maternal and newborn nutrition and health Fact Sheet. 2018,
- Braveman, P., Marchi, K., Egerter, S., Metzler, M., Stancil, T., Libet, M.,
- Poverty, near-poverty, and hardship around the time of pregnancy. Matern Child Health J., 2010. 14: p. 20–35.
- Shariff, Z.M., and Khor, G.L., Obesity and household food insecurity: evidence from a sample of rural households in Malaysia. Eur J Clin Nutr. 2005. 59: p. 1049–1058.
- Organization, W.H. Nigeria Maternal and Perinatal Health Profile. 2013 [cited 2017 April10]; Available from:
http://www.who.int /maternal_child_adolescent/epidemiology/profi les/maternal/nga.pdf.