


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Assessment of Quality of Life and Associated Factors among Patients with Schizophrenia in Ethiopia, 2017
Tolesa Fanta1,Dessie Abebaw2,Kibrom Haile3,Getahun Hibdye4,Dawit Assefa5,Tesfalem Araya6,Agitu Tadesse7
2.Public Health Specialist at Amanuel Mental Specialized Hospital Research and Training Department.
3.Chief Research and Training Director at Amanuel Mental Specialized Hospital Research and Training Department, and Psychiatrist.
4.Amanuel Getahun Hibdye is Expert Psychiatry Professional at Amanuel Mental Specialized Hospital Clinical Service Department.
5.Psychiatrist at Amanuel Mental Specialized Hospital.
6.post graduate and under graduate team leader at Amanuel Mental Specialized Hospital.
7.post graduate program coordinator at Amanuel Mental Specialized Hospital.
Copyright :© 2017 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction: The quality of life of the schizophrenic patients has been found to be impaired compared to general population. This is due to the impact of schizophrenia on the quality of life of the patients frequently entails worse functioning because of its chronicity nature of the illness , lack of fully efficacious and effective treatment, lack of awareness about the illness, public stigma and adverse effects of medication.
Objective: To assess level of quality of life and associated factors among patients with Schizophrenia in Ethiopia.
Method: Institutional based cross sectional study was conducted from January to June 2017 on patients with Schizophrenia at amanuel Mental Specialized Hospital. Single population proportion formula was used to calculate sample size and the final sample size was 423. Systematic random sampling method was used to select participants. WHOQOL-BREF was used to assess quality of life of the patients. Data was interred in to and cleaned by Epidata and exported to SPSS-20 for further analysis. Descriptive statistics was used to describe the data; OR and 95% CI was used to measure the association. P-value of less than 0.05 was used to see the statistically significance of the association.
Result: A total of 422 patients with schizophrenia were involved in the study and the response rate for the study was 99.76%. Among the participants 290(68.7%) were male. The mean age of the participants is 35.46 with + 9.25 standard deviation. The most frequently prescribed antipsychotic drug is chlorpromazine 184(43.6%) followed by Resperidone 111 (26.3%). Amitriptyline is the most frequently prescribed drug among the medications ordered for other comorbid psychiatric conditions 42(41.6%) followed by Fluoxetine 27(26.7%). The most frequently occurring chronic medical illness in this study is Diabetes Mellitus 10(43.5%) followed by Tuber Closes (TB) and Gastritis 8(34.8%). Poor quality of life is found in 48.6% of participants. Among the cofactors educational status, occupation, resperidone, depression and sexual dysfunction were significantly associated with quality of life.
Conclusion: This study shows that most of the patients with Schizophrenia are suffering from poor quality of life and need special attention. Educational status (unable to read and write), occupation (working in NGO), being on Resperidon, having depression and sexual dysfunction were significantly associated with poor quality of life.
Abbreviations: AMSH: Amanuel Mental Specialized Hospital; CSFQ: Changes in Sexual Functioning Questionnaires; PHQ-9: Patients Health Questionnaire nine; SD: Sexual Dysfunction; SMI: Severe Mental Illness; SPSS: Statistical Package of Social Science; USA: United States of America, WHOQOL: World Health Organization Quality of Life.
Quality of Life,Associated Factors among Patients,Schizophrenia in Ethiopia,Psychiatry
Schizophrenia has been characterized as one of the most severe and disabling mental illness and is found in all geographical areas [1].
The lifetime prevalence of schizophrenia is estimated to be about 1% worldwide and in Ethiopia prevalence is 0.47% [1,2]. Schizophrenia classically begins in early adulthood or late teenage years [3]. It is considered as a long-lasting disorder with poor progress and one of the major psychotic illnesses in Ethiopia [4].
Frequent hospitalization, high relapses and loss of ability to work are strongly associated with Schizophrenia. Patients with schizophrenia are also prone stigma, which leads to discrimination and thus affects their life opportunities, such as health care services, housing, education, employment and social relationships and all these leads to poor quality of life [3].
Quality of life is a dynamic concept that can change from time to time and is characterized by its individuality; each individuals perceive their quality of life as different from that of others' [5].
Based on its definition of health the World Health Organization has defined quality of life in the context of health as “individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns (3).
The quality of life of patients with schizophrenia has been found to be impaired compared to general population. This is due to the impact of schizophrenia on the quality of life (QoL) of the subject frequently entails worse functioning because of its chronic character, lack of fully efficacious treatment, lack of disease awareness, social stigma and adverse effects of treatment [6].
In treating and managing Schizophrenia, clinicians often focus on treating psychotic symptoms and ignore factors that are directly related to quality of life and prognosis of disease even though evaluation of patient’s quality of life can help a lot in improving quality of care in Schizophrenic patients [7].
In the care of patients with schizophrenia, interventions which only target symptoms are not enough, but a more holistic view is necessary in which patients’ QoL is a central concern. Even if quality of life is very important component of human being and also a target of treatment and rehabilitation in treating patients with psychiatric disorder there are limited and even no studies conducted regarding quality of life of patients with Schizophrenia in Ethiopia. So, the aim of this study was to assess the level of quality of life among patients with Schizophrenia and contributing factors to it.
2. Methodology
Study Design and Study Period: Institutional based cross sectional study was conducted from January to June 2017.
Study Area: The study was conducted at Amanuel Mental Specialized Hospital (ASMH) located in the country’s capital, Addis Ababa. Amanuel mental specialized hospital is the only mental specialized hospital in the country where patients with severe mental illness, including schizophrenia, are treated. The hospital has a case load of more than 10,000 patients per month and schizophrenia is a leading diagnosis.
Population: All patients with Schizophrenia who are on follow up at AMSH are the source populations and people with Schizophrenia in the age group 18 & above who were on treatment at AMSH during the study period were study population.
Eligibility Criteria: All patients with Schizophrenia in age group 18 and above were included in the study and the patients in exacerbation phase were excluded from the study.
Sample Size: Single population proportion formula was used to determine the minimum number of sample required for this study. Since there is no study conducted previously in our country regarding this issue, we used proportion as 50% in sample size calculation. The final sample size for this study with 10% nonresponse rate was 423.
Sampling Procedure: Systematic random sampling technique was used to select the study participants from 4,885 patients with schizophrenia came for follow up during data collection period with interval of 11th.
Study Variables: The outcome variable for this study was Quality of Life among patients with Schizophrenia. Socio-demographic factors, duration of the illness, duration on treatment, medication, comorbid known chronic medical illness, history of admission and relapse, adherence to drug, Sexual Dysfunction, Suicide, Depression and history of substance use were explanatory variables for this study.
Instruments: The gold standard instrument which is Structured Clinical Interview for DSM-ΙѴ-TR axis Ι disorders (SCID) was used to confirm a diagnosis of Schizophrenia. Quality of Life was assessed with WHOQOL-BREF which was developed by WHO and cross culturally valid instrument. It contains 26 items with four
domains: physical health (7 items), psychological health (6 items), social relationships (3 items), and environmental health (8 items). It also contains items which measure general perception of life and health (Item 1 and Item 2) This WHOQOL is probably the most widely used health-related quality of life measure in the world with about 58 national versions [8]. Each individual item of the WHOQOL-BREF is scored in Likert scale from 1(very dissatisfied) to 5 (very satisfied). Following the instructions listed in a manual on WHOQOL-BREF prepared by WHO, raw scores for the domains of WHOQOL-BREF were calculated and were transformed on the scale ranging from 0 to 100, where 100 is the highest and 0 is the lowest QOL score. The mean of each domain and the mean of total score was also calculated. Mean scores of WHOQOL-BREF was used to categorize Quality of Life as Good and Poor QOL. Hence, the subjects who scored less than or equal to mean score were categorized as having POOR QOL and those who scored greater than mean score were categorized as having GOOD QOL.
Sexual dysfunction was measured by using Changes in Sexual Functioning Questionnaires (CSFQ-14). PHQ-9 and 8 –item Morisky medication adherence Scale were used to measure depression and medication adherence respectively. The English version of the instruments was translated to local language and was back retranslated to English by professionals in subject matter.
Data Quality Control: 17 masters level mental health students were hired for data collection and two masters level mental health professionals were hired to supervise the data collectors. The data collectors were given a one day training on questionnaire and way of assessment. Pre-test was conducted two weeks before the start of actual data collection to know the time needed to complete one questionnaire and to know whether the questionnaire used is understandable to the study participants or not. The data collected during the pre-test was not included in the final analysis.
Data Processing and Analysis: Data was coded and entered to Epi data and transferred to Statistical Package for Social Sciences version 20 (SPSS-20) for further analysis. Descriptive statistical analysis was used to estimate the frequencies and percentages of the variables. Bivariate and multivariate logistic regression analysis was used to see the association between outcome and explanatory variables. The strength of the association was measured by odds ratio with 95% CI and P-value less than 0.05 was considered as statistically significant.
Ethical Consideration: Ethical clearance was obtained from AMSH Ethical Review Committee. The Four Item Abbreviated Mental Test (AMT4) was used to measure the capacity of the patient to give consent. Then the purpose, importance and confidentiality of the information gathered was explained to each of the competent participant before the start of interview. Participants were also informed that there is no harm to them if they would not agree to participate or withdraw from participation during the data collection process. Finally, their willingness to be involved in the study was asked and written consent was obtained. At the time of data collection the investigator, supervisor and data collectors followed ‘code of ethics’ and obeyed the rules & regulations of the hospital. Privacy was kept strictly at the time of data collection.
3. Result
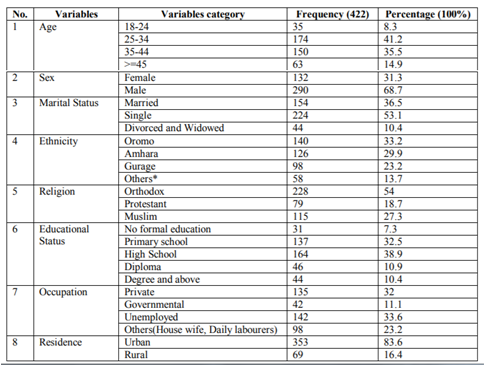
A total of 422 patients with schizophrenia were involved in the study and the response rate for the study was 99.76%. Among the participants 290(68.7%) were male. The mean age of the participants is 35.46 with + 9.25 standard deviation. Majority of the participants 353(83.6%) were from urban area (Table 1).
4. Medication Related Factors
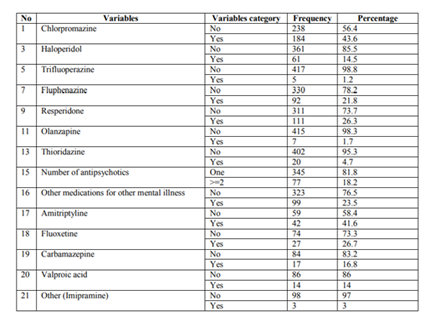
The most frequently prescribed antipsychotic drug is chlorpromazine 184(43.6%) followed by Resperidone 111 (26.3%) (Fig. 1). Amitriptyline is the most frequently prescribed drug among the medications ordered for other comorbid psychiatric conditions 42(41.6%) followed by Fluoxetine 27(26.7%) (Table 2).
5. Clinical Factors And Substance Related Factors
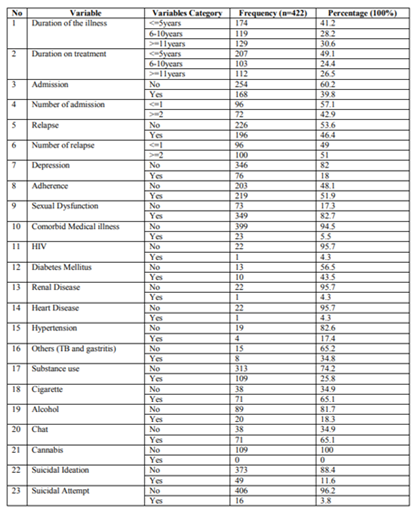
The most frequently occurring chronic medical illness in this study is Diabetes Mellitus 10(43.5%) followed by Tuber Closes (TB) and Gastritis 8(34.8%). (349)82.7% of the study participants have sexual dysfunction. Among the substance users 71(65.1%) use cigarette and 71(65.1%) use khat. The median score of duration of the illness (Table 3) is 7 with inter quartile range of 6, and the median score of duration on treatment is 6 with inter quartile range of 10. The median score for frequency of admission is 1 with inter quartile range of 1, and the median score for frequency of relapse is 2 with inter quartile range of 2.
6. Magnitude Of Quality Of Life Among Patients With Schizophrenia
The mean score of the WHOQOL-BREF scale in this study was 60.6 with Standard Deviation of + 9.13. Out of the total 422 study participants, 48.58% had poor quality of life. The WHOQOL BREF also covers four different domains of quality of life (physical Domain, psychological Domain, social Domain and environmental Domain) (Table 4) (Figure. 1).


7. Bivariate And Multivariate Analysis
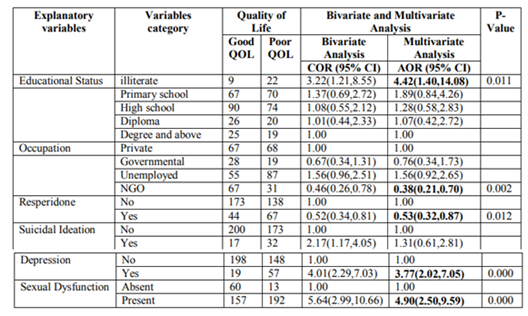
After bivariate logistic regression analysis, six variables (Educational status, Occupational Status, Resperidone use, Suicidal Ideation, Depression and Sexual Dysfunction) met the requirement to proceed to multivariate logistic regression analysis. After multivariate analysis, Educational status, Occupational status, Resperidone use, Depression and Sexual Dysfunction were significantly associated with Poor Quality of Life. Compared to those who are degree and above holders, being illiterate, [AOR 4.44, 95% CI (1.40, 14.08)] were significantly associated with Quality of life. Working in NGO, [AOR 0.38, 95% CI (0.21, 0.70)], being on Resperidone, [AOR 0.53, 95% CI (0.32, 0.87)], Depression, [AOR 3.77, 95% CI (2.02, 7.05)] and Sexual Dysfunction, [AOR 4.90, 95% CI (2.50, 9.59)] were significantly associated with Quality of Life at p-value< 0.05 (Table 5).
8. Discussion
This study found that quality of life of patients with Schizophrenia is extremely impaired and needs attention. In this study 48.6% of the study participants scored less than mean score of WHOQOL-BREF which was labeled as poor quality of life. This finding is less than that of Brazil (93%) and that of Nigeria (11.2%) [9]. This discrepancy may be due to difference in sample size (160 in case of Nigeria and 181 in in case of Brazil), tool difference (QLS-BR in case of Brazil) and difference in cultural back ground.
In multivariate analysis, after adjusting for possible confounding factors, participants who are unable to read and write are 4.42 times more likely to have poor quality of life compared to those who are degree and above [4.42(1.40,14.08)]. This finding is supported by study conducted in Latin America on schizophrenic patients and study conducted in Ethiopia on Epileptic patients [10,11].
The participants who employed in NGO are 62% protective against having poor quality of life [0.38(0.21, 0.70)] compared to those who are in private work. This finding is supported by the study conducted in Brazil [12].
Being on Resperidone is 47% protective against having poor quality of life [0.53(0.32, 0.87)] compared to those who were not on Resperidone. This finding is supported by the finding of research conducted in Spain in which the participants those who were on second generation antipsychotics became protective against having poor quality of life [13].
The participants who screened positive for depression are 3.8 times more likely to have poor quality of life compared to those who screened negative for depression. This finding is supported by the study conducted in Finland, Japan and Nigeria. This may be due to [3,14,15].
The participants who have sexual dysfunction are 4.9 times more likely to have poor quality of life compared to those who have no sexual dysfunction [4.90(2.50,9.59)]. This result is supported by the study conducted by Olfson and Kandrakonda S [16]. This may be due to the fact that an inproper sexual functioning may affect maintaining a satisfying intimate relationship which is the major component of Quality of life.
9. Conclusion
This study shows that most of the patients with Schizophrenia are suffering from poor quality of life and need special attention. Among the hypothesized factors to be risk factors for poor quality of life, educational status (unable to read and write), occupation (working in NGO), being on Resperidon, having depression and sexual dysfunction were significantly associated with poor quality of life.
10. Declarations
Acknowledgements
We are grateful to the data collectors and supervisors for their unreserved effort. Our gratitude also goes to Amanuel Mental Specialized Hospital for funding this study. Finally we are grateful to the study participants for their patience.
Funding
Funding for this study was provided by Amanuel Mental Specialized Hospital.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Authors’ Contributions
TF involved in designing and coordinating overall progress of the study; KH, DA2, GH, DA5, TA and AT equally contributed in the design of the study, performed the statistical analyses and critically revised the manuscript. All authors read and approved the final manuscript.
References
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. American journal of respiratory and critical care medicine. 2001 Apr 1; 163(5):1256-76.
- Teferra Abebe S. Studies on psychotic disorders in rural Ethiopia (Doctoral dissertation, Umeå University).
- Pitkänen A. Improving quality of life of patients with schizophrenia in acute psychiatric wards.
- Shibre T, Negash A, Kullgren G, Kebede D, Alem A, Fekadu A, Fekadu D, Medhin G, Jacobsson L. Perception of stigma among family members of individuals with schizophrenia and major affective disorders in rural Ethiopia. Social psychiatry and psychiatric epidemiology. 2001 Jun 1; 36(6):299-303.
- ELhay ES, Mona A, Mohamed H. The Effect of Auditory Hallucinations Management Program on Quality of Life for Schizophrenic Inpatients, Egypt.
- Medeiros-Ferreira L, Obiols JE, Navarro-Pastor JB, Zúñiga-Lagares A. Metabolic syndrome and health-related quality of life in patients with schizophrenia. Actas Esp Psiquiatr. 2013 Jan 1; 41(1):17-26.
- Gaur V, Jagawat T, Gupta S, Khan PA, Souza MD, Sharan A. Quality of life in outpatient schizophrenics: correlation with illness severity and psychopathology. Delhi Psychiatry Journal. 2015; 18(1):95-101.
- Whoqol Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological medicine. 1998 May; 28(3):551-8.
- Lasebikan VO, Owoaje ET. Quality of life in psychosis: prevalence and associated factors in a Nigerian clinical population. Community mental health journal. 2015 May 1; 51(4):491-6.
- Caqueo-Urizar A, Urzúa A, Boyer L, Williams DR. Religion involvement and quality of life in patients with schizophrenia in Latin America. Social psychiatry and psychiatric epidemiology. 2016 Apr 1; 51(4):521-8.
- Tegegne MT, Muluneh NY, Wochamo TT, Awoke AA, Mossie TB, Yesigat MA. Assessment of quality of life and associated factors among people with epilepsy attending at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia. Science Journal of Public Health. 2014; 2(5):378-83.
- Silva TF, Mason V, Abelha L, Lovisi GM, Cavalcanti MT. Quality of life assessment of patients with schizophrenic spectrum disorders from Psychosocial Care Centers. Jornal Brasileiro de Psiquiatria. 2011; 60(2):91-8.
- Alonso J, Croudace T, Brown J, Gasquet I, Knapp MR, Suárez D, Novick D. Health-related quality of life (HRQL) and continuous antipsychotic treatment: 3-year results from the Schizophrenia Health Outcomes (SOHO) study. Value in Health. 2009 Jun 1; 12(4):536-43.
- Kunikata H, Mino Y, Nakajima K. Quality of life of schizophrenic patients living in the community: The relationships with personal characteristics, objective indicators and self‐esteem. Psychiatry and Clinical neurosciences. 2005 Apr 1; 59(2):163-9.
- Lasebikan VO, Owoaje ET. Quality of life in psychosis: prevalence and associated factors in a Nigerian clinical population. Community mental health journal. 2015 May 1; 51(4): 491-6.
- Kandrakonda S, Jally MR, Kesava Reddy SR, Miryala G. Prevalence of sexual dysfunction in patients with mental illness receiving psychotropic medication. AP J Psychol Med 2014; 15(2):235-39.