


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
ARC Journal of Nursing and Healthcare
Volume-1 Issue-1, 2015
Abstract
Immunization coverage in Bida Emirate Area (BEA) is still very low in spite of the huge financial resources expended in Nigeria.This however, raises concerns as to what could be responsible. This study aimed at assessing the effects of mothers' knowledge, attitude and practice (KAP) on immunization coverage in the rural communities of BEA of Niger state. Chi square was used to determine the effect of KAP and multiple logistic analyses was used to determine the likelihood effects of these factors on immunization status.The full immunization (FI) coverage was 27.81%. The study revealed that the percentage of those who had considerable knowledge of: number of times OPVs are given, the age of the child at which MCV is given and BCG preventable symptoms were significantly higher for those who have their children completely immunized. The low literacy level in these rural communities may be responsible for the very low KAP of mothers recorded, which also may have contributed to the very low immunization status. We recommended among others that girl child education is given more priority over early marriage in this area as well as increased rural community mobilisation and participation for both men and women in immunization services.
2.KEYWORDS
3.INTRODUCTION
4.DATA AND METHODS
5.RESULTS AND FINDINGS
6.DISCUSSION
7.REFERENCES
AUTHOR DETAILS
Obasohan, Phillips Edomwonyi1; Anosike, Bernard Ubannache2, Etsunyakpa, Mohammed Busu3
1,2Department of General and Liberal Studies College of Administrative and Business Studies,
Niger State Polytechnic, Bida Campus, Bida, Niger State, Nigeria
3Department of Social Welfare Administration College of Administrative and Business Studies,
Niger State Polytechnic, Bida Campus, Bida, Niger State, Nigeria
For Correspondence: [email protected]
KEYWORDS
Knowledge, Attitude, Practice, Immunization, Vaccination, Coverage, Bida Emirate, Rural
INTRODUCTION
It is reported that over 3 million deaths occur worldwide every year from Vaccine Preventable Diseases (VPDs) and over 2 million deaths are delayed through immunization processes [1, 2, 3]. The implication is that more childhood mortality resulting from VPDs is still being recorded than are being prevented by vaccines [3]. However, immunization of children remains one of the most cost effective and public health intervention strategies to combat childhood morbidity and mortality arising from infectious diseases [1, 3, 4, 5]. In Nigeria for instance, under-five mortality rate ranks as one of the highest worldwide and VPDs account for more than 22% of these deaths [6] amounting to over 200,000 deaths per year [7].
A recent guideline by World Health Organization (WHO), United Nations Children's Fund (UNICEF) and National Programme on Immunization (NPI) which was adopted for Nigeria and began in Niger State in February, 2013 stipulates that a child should receive four doses of OPV (Oral Polio Vaccine), three doses of Pentavalent vaccines (a combination of five vaccines-in-one that prevents diphtheria, tetanus, whooping cough, hepatitis B and haemophilus influenza), and one dose each of BCG (Bacilli Calmette- Guerin), HEPB 0, MCV (Measles Containing Vaccine) and Yellow Fever [3, 7, 8]. To effectively control VPDs therefore is a function of the extent of immunization coverage achieved. This explains the fact that poor immunization coverage accounts for greater burden of VPDs especially in the rural areas [9].
Many factors (individual, community and systematic) have been found to be responsible for low vaccination coverage in most parts of the world especially in the developing countries [10]. Some studies have shown consistent association between mother's literacy level and immunization status of children. Literate mothers perhaps had basic knowledge about the purpose of immunization. In the same way, complete immunization coverage was found to be associated with the parent's level of education, for instance, children of non-educated fathers who reported no knowledge of the objectives of immunization were less likely to be completely immunized [11].
Studies have revealed that under-five mortality is inversely related with their immunization coverage rates, but however it varied between developed and developing countries [9]. For instance, advanced countries with under-five mortality rate of less than 10 in a 1000 have more than 90% immunization status. However, in developing countries with immunization coverage rates below 80% have underfive mortality rates above 100 in a 1000 [9, 12]. So, strengthening national immunization systems, especially in countries with the greatest number of under-vaccinated children, should be a global priority to reduce morbidity and mortality from vaccine-preventable diseases [8].
For a child to be fully immunized in Nigeria it cost as much as $226 (Two Hundred and Twenty Six Dollars) per child, the most expensive among developing countries [9]. In spite of these huge resources being expended, surprisingly has not resulted to significant increase in immunization coverage in the country. The percentage of fully immunized children in Nigeria has marginally increased from 13% in 2003 to 23% in 2008 [2, 9, 13] and only slightly increased to 25% in 2013 [14]. This however raises concerns as to what could be responsible. The purpose of this study among others is to determine the immunization status/coverage of children aged 12 – 24 months and assess the maternal/care givers' knowledge, attitude and practice (KAP) of its processes in the rural communities of BEA of Niger state.
DATA AND METHODS
Survey design
A community-based cross-sectional data from a previous descriptive survey [3] was used in this study. BEA has six Local Government Areas (LGA), one of the LGA is purely an urban community. From the remaining 5 LGA's, the sampling frame of the districts was obtained (excluding the districts hosting the LGA headquarters) and were considered as clusters. A systematic random sampling was adopted to select representative sample cluster districts by selecting every second district resulting into 19 districts. All the major villages under the selected 19 districts were given equal chance of been selected to be the starting village in their district using a simple ballot. From the selected village, all eligible mothers were interviewed. At the event where we were unable to find the total needed for the cluster, the nearest village was considered and so on till the required number of respondents were found [5, 15].
Survey Instrument
The survey collected information on socioeconomic, demographic and immunization indicators from a representative sample of 495 mothers of eligible children of age 12 – 24 months in these rural communities in BEA, as well as the mother's basic knowledge, attitude and practice of immunization processes. The study also elicited information on the child's immunization status whether they were fully, partially or not immunized at all. The child's immunization card was examined and where not available, the mother was asked to give the history of the immunization.
Ethical Approval
The ethical approval for this project was given by the Research and Development Committee of Niger State Polytechnic in Zungeru. We also obtained informed consent from the Administrative Heads of the localities where data were collected and from all respondents who participated in the survey before the interview was conducted. A Parting gift of Paracetamol syrup was given to each mother who consented to participate in the survey [3].
Variables of Interest
Outcome Variable: The outcome variable was the immunization status of the children age 1224months obtained from the child's immunization card (or by history) and classified as: '1' if the child had been fully immunized of all the basic doses of BCG, OPV0 and HEPB0 at birth, 3 doses each of OPV and Pentavalent, 1 dose each of MCV (Measles Containing Vaccine) and Yellow Fever Vaccine; classified as: '0' if the child had missed any of these doses or had not even been immunized at all.
Exposure Variables: The main explanatory variables were the knowledge, attitude and practice of immunization processes; the socioeconomic and demographic characteristics of the mothers and fathers, as well as some child's factors.
Statistical Analyses
We adopted the following levels of data analysis:
(i) Bar charts were used to describe the immunization status of children
(ii) We examined the independent relationship between selected KAP variables and immunization status using chi-square test and 95% Confidence Interval.
(iii) To further examine how 'KAP' influence child's immunization status, three different models were fitted.
- Unadjusted univariate logistic analysis of the effect of KAP on immunization status
- Unadjusted multivariate logistic analysis of the effect of KAP on immunization status
- Adjusted multivariate logistic analysis of the effect of KAP incorporating other background variables at multivariate level.
RESULTS AND FINDINGS
Background Variables
The average age of mothers who participated in the survey was 29 years with standard deviation of 6 years and that of the of the children was 17 years with standard deviation of 4 years. Only 0.81% were of Christian faith and the rest were Muslims. About 93% of the respondents are below secondary school education. Majority of the respondents are into farming and trading (89%). 204 representing 41% were children of fourth order and above, while 98 (20%) were of the first order. Majority of our respondents were in a monogamous marriage (50%), of 40%, their partner has two wives, 8% with three wives and 2.2% with either four wives or above. About 42% of the respondents, their partners do not have education, 13% went to primary school, 27% had secondary education, while only 16% had higher education. 53% of the respondents delivered the baby concerned in a health facility and 44% delivered at home
Immunization Status
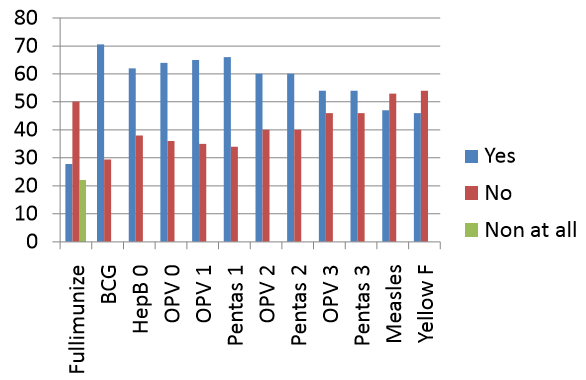
The study showed that full immunization (FI) coverage of children between 12 to 24 months in rural communities in BEA was 27.81%, partial immunization (PI) was 50.10% (i.e. had received at least one of the doses of immunization, but not all) and 22.09% had never been immunized at all, and 33.88% do not have immunization card.
It was observed that 71% of children age 12-24months in rural communities of BEA have received BCG vaccination, 62% received Hep B 0 and 64% have had OPV0. Only 54% were immunized with OPV3 resulting to a dropout rate of 10% in OPV0 to OPV3. In the same way, 66% of these children were immunized with Pentas 1, Pentas 2 (54%) and 55% have had Pentas 3 bringing about 11% dropout rate; 53% and 54% could not be immunized with Measles Containing Vaccines and Yellow Fever Vaccine respectively.
Multiple Bar Chart representing the immunization status in percentage.
Relationship between KAP and Immunization Status of Children.
Table 1 shows the effects of KAP on immunization status. It revealed that the percentage of those who had knowledge of: number of times OPVs are given, the age of the child at which MCV is given and BCG preventable symptoms are significantly higher for those who have their children completely immunized. Among those who had negative attitude on: the benefit of immunization, will not recommend immunization for others and are not ready to pay for immunization if asked to, were significantly higher among those who had incomplete immunization status. Having a card was found to be significantly associated with immunization status. The place where immunization is obtained was also significantly associated with the immunization status
Unadjusted Logistic Analysis of KAP and Immunization Status
Table 2 shows the unadjusted multivariate logistic analysis of the effects of KAP on immunization status. The odds of immunization of child for those who knew the purpose of immunization is 6.7 times higher than those who have no knowledge of the purpose. The odds of immunization for those who knew the BCG preventable disease and the age at which a child will complete his/her immunization are 5 and 2 times respectively significantly higher than those who do not know. For those who believed that immunization is beneficial the odds of immunizing their children were 7 times higher than the reference group (those who said is not beneficial).
**p< 0.05; UIOR=Unadjusted Independent Odd Ratios; UMOR=Unadjusted Multivariate Odd Ratios and AOR=Adjusted Odd Ratios
Effects of KAP on immunization status after adjusting for cofounding socioeconomic and demographic variables
After adjusting for cofounding socioeconomic and demographic factors using multivariate logistic analysis (Model 3 of table 2), we observed that only the factors such as 'knowing the purpose of immunization', 'believed that immunization is beneficial', 'the child had immunization card', that 'immunization can be taken in the health facility', the 'child is of a higher birth order', and 'respondents' partner hold a primary education level', were found to significantly increased the chance of complete immunization compare with their reference group. However, those who claimed that they would recommend immunization for others were surprisely found to significantly decrease the chance of complete immunization coverage.
Test for Goodness of Fit and Multicollinearity
We conducted Likelihood Ratio Test (LHRT) to test for goodness of fit between the effects of unadjusted KAP on immunization Status and that of KAP after adjusting for socioeconomic and demographic variables. The chi square was 25.26 with degree of freedom 23 and the p=value of 0.3369 indicating that there was no statistical significant improvement in the model fit (That is adjusted KAP is not different from the unadjusted KAP on immunization status). Also, we performed a test of multicollinearity using Variance Inflation Factor (VIF) and the values ranged from 1.13 to 4.67 with a mean VIF of 2.52 indicating that there was no case of multicollinearity since VIF were all less than 10 [16].
DISCUSSION
The Immunization Coverage of children in Rural BEA of Niger State, Nigeria
The 28% full immunization status for children in rural communities of BEA is relatively very low. This is however, comparable to 30% found for the whole BEA which was reported elsewhere [3] and in a rural community in southwestern Nigeria [9], and is just a little higher than national coverage of 25% achieved in 2013 [13]. However, the 10% drop out recorded for OPV0 to OPV3 is within the acceptable benchmark [9], this was lower than what was found for the entire region, indicating that mothers in rural areas were more consistent in immunizing their children than anywhere else in the region. Also, the dropout rate for Pentas of 11% is just 1% above acceptable benchmark, but is however lower than what was recorded in the whole of BEA [3]. The probable reasons for these dropouts and low immunization status recorded may not be unconnected with non-availability of the vaccines on equal basis. Also, OPVs are taken orally and Pentas are injectables, there is the likelihood that mothers in the rural areas may be more skeptical about the side effects of injectables than of oral.
The Effects of KAP of immunization processes on Immunization Status
The KAP of mothers/care givers have a direct significant effect on the immunization status of the children. Greater percentage of those who do not have correct knowledge of: purpose of immunization, number of times OPVs are given, at what age Measles Containing Vaccine is taken, the side effect of vaccines taken at birth and the age at which vaccination is completed were significantly greater among those whose children were incompletely immunized than those completely immunized. This agrees with other findings [18]. Also the attitudes the mothers have toward immunization exercise have direct effects on immunization status.
However, after adjusting for the significant cofounding socioeconomic variables, knowing the purpose of immunization was still significant, which agrees with the popular saying that 'when the purpose of a thing is not known, abuse is inevitable'. The low literacy level in these rural communities may be responsible for the very low KAP of mothers recorded, which also may have contributed to the very low immunization status. The child having an immunization card has a direct relationship with the immunization status. An immunization card could often serve as reminder/motivator to go for immunization
CONCLUSION AND POLICY RECOMMENDATIONS
Our conclusion in this study is that full immunization coverage of children in rural communities of BEA is very low compare with the expectation of WHO of 80% full immunization coverage in subregion as at 2010. This status is not unconnected with very poor KAP of mothers/care givers on immunization processes which in turn is traceable to very high illiteracy level especially in the rural areas.
The findings from this study have far reaching policy implications as such; we put forth the following recommendations:
- Girl child education should be encouraged at the expense of early marriage especially in the rural areas.
- An increased rural community mobilization and participation of both men and women in immunization services
- Increase in advocacies by health workers on the purpose and need for immunizing children against preventable deadly diseases.
- These advocacies could also be directed not only to the mothers alone but also to the fathers thereby increasing men's participation in reproductive health
- All health workers posted to rural health centres should be encouraged to live in the communities they are posted to work.
- Health centres be equipped with solar powered refrigerators for preservation of the vaccines
- All children eligible for Immunization should be issued cards. In a situation where it is misplaced, effort should be made to have it replaced.
This study was sponsored by Tertiary Education Trust Fund (TetFund), Nigeria, through the intervention funds under the Institution Based Research Grant (IBR) with reference number: TETFUND/DESS/POLY/ZUNGERU/RP/VOL. II.
REFERENCES
- Odusanya OO, Alufohai EF, Meurice FP and Ahonkhai VI. Determinants of Vaccination Coverage in Rural Nigeria BMC Public Health. 8:381 (2008) doi:10.1186/1471-2458-8-381.
- Centre for Global Development. Making Markets for vaccines: from ideas to actions. Centre for Global Development, Washington DC. (2005)
- Obasohan PE, Anosike BU aand Etsunyakpa MB. Determinant of Full Immunization Coverage and Reasons for its Failure for Children in Bida Emirate Area, Niger State, Nigeria. Merit Research Journal of Medicine and Medical Sciences; 3(10), 476-483 (2015).
- Odusanya OO, Alufohai JE Meurice FP, Clemens R and Ahonkhai VI. Short Term Evaluation of a Rural Immunization Program in Nigeria; Journal of the National Medical Association. 95(2): 175 – 179 (2003)
- World Health Organization. Immunization, Vaccines and Biologicals. Retrieved on 11th Dec 2014 from http://www.who.int/immunization/en/
- Itimi K, Dienye PO and Ordinioha B. Community participation and Childhood immunization Coverage:A Comparative Study of Rural and Urban Communities of Bayelsa State, South-South, Nigeria. Nigerian Medical Journal, Vol. 53 Issue 1, 21-25 (2015).
- Nigerian Immunization Schedule. http://www.mamalette.com accessed 15/08/2015
- Centre for Disease Control and Prevention. Global Routine Vaccination Coverage-2012 Morbidity and Mortality Weekly Report (MMWR). November 1, (2013) 62(43); 858-861.
- Adebayo BE, Oladokun RE and Akinbami FO. Immunization Coverage in Rural Community in Southwestern Nigeria; Journal of vaccines and Vaccination. 3:143. (2012) Doi:10.4172/21577560.1000143.
- Antai D. Rural-Urban Inequalities in Childhood Immunization in Nigeria: The Role of Community Contexts; African Journal of Primary Health Care and Family Medicine, Vol. 3, No 1 (2011).
- Sanou A, Simboro S, Kouyaté K, Dugas M, Graham J and Bibeau G. Assessment of factors associated with complete immunization coverage in children aged 12-23 months: a crosssectional study in Nouna district, Burkina Faso; BMC International Health and Human Rights. 9(Suppl 1):S10 (2009) doi:10.1186/1472-698X-9-S1-S10.
- Bida Emirate. 19.18 UTC. In Wikipedia: The Free Encyclopedia. Wikimedia Foundation Inc. Encyclopedia on-line. Retrieved on 05 June, 2015 from http://en.wikipedia.org/wiki/ bida_emirate.
- National Population Commission and ICF Macro. Nigeria Demographic and Health Survey 2013. Abuja, Nigeria: National Population Commission and ICF Macro (2009).
- National Population Commission and ICF Macro. Nigeria Demographic and Health Survey 2013. Abuja, Nigeria: National Population Commission and ICF Macro (2014).
- Etana B and Deressa W. Factors Associated with Complete immunization Coverage in Children Aged 12 – 23 months in Ambo Woreda, Central Ethiopia; BMC Public Health. 12:566 doc:10.1186/1471-2458-12-566. (2012)
- Kayode GA, Adekanmbi VT and Uthman OA. Risk Factors and a Predictive Model for Under-Five Mortality in Nigeria: Evidence from Nigeria Demographic and Health Survey; BMC Pregnancy and Childbirth. 12:10 (2012)
- StataCorporation. Stata Statistical Software, College Station, TX: (2014)
- Maekawa M, Douangmala S, Sakisaka K, Takahashi k, Phathammavong O, Xeuatvongsa A and Kuroiwa C. Factors Affecting Routine Immunization Coverage among Children Aged 12 – 59 months in Lao PDR after Regional Polio Eradication in Western Pacific Region; BioScience Trends; 1(1): 43 – 5, (2007)1
AUTHORS BIOGRAPHY
 Obasohan Phillips Edomwonyi, was born on the 16th June, 1961. He obtained a B. Sc (Hons) Industrial Mathematic in 1987; Master in Educational Measurement and Evaluation in 1994 and Masters in Business Administration (MBA) in 1997, all from the University of Benin, Nigeria. To further strengthen his academic delivery coupled with his love for interdisciplinary areas, he attended University of Birmingham, United Kingdom and obtained Masters of Science degree (M. Sc) in Mathematics, Operations Research, Statistics and Econometrics (MORSE) in 2012. He is an academic staff with Niger State Polytechnic, Zungeru, Nigeria and rose to the rank of Chief Lecturer in 2006. Obasohan Phillips loves research (especially, empirical) and was recently the Principal Researcher in a TetFund (Nigeria) sponsored Institution Based Research Grant (IBRG) which has been concluded. He is a Fellow and current National President/Chairman of Council of the Institute for Operations Research of Nigeria (INFORN).
Obasohan Phillips Edomwonyi, was born on the 16th June, 1961. He obtained a B. Sc (Hons) Industrial Mathematic in 1987; Master in Educational Measurement and Evaluation in 1994 and Masters in Business Administration (MBA) in 1997, all from the University of Benin, Nigeria. To further strengthen his academic delivery coupled with his love for interdisciplinary areas, he attended University of Birmingham, United Kingdom and obtained Masters of Science degree (M. Sc) in Mathematics, Operations Research, Statistics and Econometrics (MORSE) in 2012. He is an academic staff with Niger State Polytechnic, Zungeru, Nigeria and rose to the rank of Chief Lecturer in 2006. Obasohan Phillips loves research (especially, empirical) and was recently the Principal Researcher in a TetFund (Nigeria) sponsored Institution Based Research Grant (IBRG) which has been concluded. He is a Fellow and current National President/Chairman of Council of the Institute for Operations Research of Nigeria (INFORN).
 Anosike, Bernard Ubannache, was born on 28th December, 1959. He hails from Oru-East Local Government Area in Imo State, South East Nigeria. He graduated from the University of Jos, where he obtained B.A (Hons) Economics/Educational Planning. Additional qualifications obtained include: PGD in Business Management Technology from Federal University Technology, Minna; Masters in Educational Planning from National Open University of Nigeria (NOUN). He is currently a Chief Lecturer in the Department of General and Liberal Studies, Niger State Polytechnic, Zungeru. He served as co-researcher in a Tetfund (Nigeria) sponsored Institution Based Research Grant (IBRG) which has been concluded. Mr Anosike is a member of Institute of Registered Administrators of Nigeria and married with children.
Anosike, Bernard Ubannache, was born on 28th December, 1959. He hails from Oru-East Local Government Area in Imo State, South East Nigeria. He graduated from the University of Jos, where he obtained B.A (Hons) Economics/Educational Planning. Additional qualifications obtained include: PGD in Business Management Technology from Federal University Technology, Minna; Masters in Educational Planning from National Open University of Nigeria (NOUN). He is currently a Chief Lecturer in the Department of General and Liberal Studies, Niger State Polytechnic, Zungeru. He served as co-researcher in a Tetfund (Nigeria) sponsored Institution Based Research Grant (IBRG) which has been concluded. Mr Anosike is a member of Institute of Registered Administrators of Nigeria and married with children.
 Etsunyakpa Mohammed Busu was born in Busu, a village in Lavun Local Government Area of Niger State, Nigeria on 27th December, 1962. Started western education with formal enrolment with primary school in 1971 and obtained General Certificate of Education Ordinary Level in 1982. Joined the services of Niger State Government in 1986 as a Social Welfare Assistant and rose to its peak before finally joining academics in which he is presently a Lecturer 1. Etsunyakpa have acquired several certificates in Social Welfare; Diploma in Social Administration and B. Sc Sociology. Presently he is pursuing a Master Degree in Sociology, seeking to specialize in Social Problems. He served as co-researcher in a Tetfund (Nigeria) sponsored Institution Based Research Grant (IBRG) which has been concluded. He is a member of the Nigerian Association of Social Workers (NASOW). Happily married with children.
Etsunyakpa Mohammed Busu was born in Busu, a village in Lavun Local Government Area of Niger State, Nigeria on 27th December, 1962. Started western education with formal enrolment with primary school in 1971 and obtained General Certificate of Education Ordinary Level in 1982. Joined the services of Niger State Government in 1986 as a Social Welfare Assistant and rose to its peak before finally joining academics in which he is presently a Lecturer 1. Etsunyakpa have acquired several certificates in Social Welfare; Diploma in Social Administration and B. Sc Sociology. Presently he is pursuing a Master Degree in Sociology, seeking to specialize in Social Problems. He served as co-researcher in a Tetfund (Nigeria) sponsored Institution Based Research Grant (IBRG) which has been concluded. He is a member of the Nigerian Association of Social Workers (NASOW). Happily married with children.