


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Prevalence of Hepatitis B Virus among Patients Diagnosed with Liver Cirrhosis Disease in Kano, Northern Nigeria
Zage A.U1, Waiya S.A2, Ali M3*, Garba M1, Muhammad A.A1
2.School of Hygiene Kano, Nigeria.
3.Department of Biological Sciences, Federal University Gusau, Nigeria.
Copyright : © 2018 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Liver cirrhosis is a common cause of morbidity and mortality worldwide and an important burden on the health care system. The present study was aimed to determine the prevalence of hepatitis B virus among patients diagnosed with liver cirrhosis disease in Kano, Northern Nigeria. A total of 37 blood samples were collected from patients diagnosed with cirrhosis liver disease attending Department of Medicine, Aminu Kano Teaching Hospital (AKTH) from June 2016 to December, 2016. Hepatitis B virus was determined using Gold Rapid Screen test with an enzyme-linked immunosorbent assay (ELISA) kits. The level of Alanine Amino-transferase (ALT), Aspartate Amino-transferase (AST), Alkaline Phosphatase (ALP) and bilirubin in the blood serum were analyzed using kits. The results indicated that 20 (54%) out of 37 cirrhosis diagnosed patients were infected with hepatitis B virus. The prevalence of hepatitis B infection among cirrhosis diagnosed patients based on age group showed that age category 41-50 years has the highest infection rate with total of 8 subjects (40%). The result also revealed that the hepatitis B infection is higher among male patients with total of 13 subjects which accounted for 65% than female patients with 7 subjects (35%). There is considerable statistical difference in the prevalence of hepatitis B infection among age categories, but no statistical differences found between male and female subjects at p< 0.05. It is concluded that hepatitis B virus is one of the most common cause of liver cirrhosis.
Cirrhosis, hepatitis, infection, Kano, liver, Prevalence,Immunology and Vaccines
1. Introduction
Hepatitis B virus (HBV) is a DNA virus of the family Hepadnaviridae and the causative agent of hepatitis B infection. Hepatitis B is one of the most common infectious diseases in the world and a major health problem. According to the most recent World Health Organization estimate, 2 billion people worldwide have serologic evidence of past or present HBV infection, and 350 million are chronically infected and at risk for HBV-related liver disease[1]. It is 50 to 100 times more infectious than HIV and 10 times more infectious than hepatitis C virus (HCV) with many carriers not realizing they are infected with the virus. It is an important cause of liver diseases such that chronic infection with HBV is a common cause of death associated with liver failure, cirrhosis and liver cancer[2].
The virus has caused severe endemic in parts of Africa and Asia[3]. The prevalence of HBV varies between 2% in developed countries where the prevalence is low to about 8% in developing countries where infection is endemic with sex, age and socio-economic status as important risk factors for infection[4]. The degree of HBV endemicity often correlates with predominant mode of transmission. The disease has an enormous impact on health and national economy of many countries and the severity of the disease is highly variable and often unpredictable. The minimum infectious dose is so low that such practices like sharing of tooth brush or a razor blade can transmit infection[5].
Cirrhosis is the common end result of chronic damage to liver parenchyma caused by a variety of liver diseases. It results in replacement of liver tissue by fibrotic scar tissue and regenerating nodules, leading to progressive liver dysfunction and clinical complications such as portal hypertension, hepatocellular carcinoma (HCC), liver failure and death. Cirrhosis is a major cause of mortality and morbidity worldwide and represents an important burden on healthcare resources [6]. All chronic liver diseases are characterized by their capacity to progress into cirrhosis. The fibrogenic process goes through various phases where excessive collagen deposition results in qualitative and quantitative changes of the extracellular matrix [7]. Cirrhosis is the structural subversion of the liver with the formation of regenerative nodules and it represents the late-stage liver disease. Advanced cirrhosis is a condition with limited treatment options. Changes in mortality for cirrhosis in different countries reflect differences in the prevalence of risk factors such as alcohol abuse and HBV and HCV infection [8]. In 2010, liver cirrhosis was the 23rd cause of death worldwide (31 million), Disability Adjusted Life Years with roughly equal proportions attributable to HCV, HBV and alcohol consumption [9]. Although cirrhosis is predominantly of viral etiology, with the current encoding system it is not possible to identify cases of cirrhosis of viral etiology [10].
Majority of liver cirrhosis is caused by viral hepatitis, excessive alcohol consumption and non alcoholic fatty liver disease (NAFLD)[11]. In resource poor countries with the burden of infectious agents, most cases of cirrhosis are due to viral hepatitis especially hepatitis B and C viruses [12,13]. However, Okeke et al in Jos Nigeria reported that most of their cases (75.6%) were associated with excessive consumption of locally brewed alcoholic beverage [14]. The present study was aimed to determine the prevalence of hepatitis B virus among patients diagnosed with liver cirrhosis disease in Kano, Northern Nigeria.
2. Materials And Methods
The study was conducted at Aminu Kano Teaching Hospital (AKTH) Kano. Kano state is located in the North-west Nigeria with coordinates 110 30 N 80 30 E. It shares borders with Kaduna state to the south- west, Bauchi state to the South-East, Jigawa state to the East, Katsina state to the West and Niger republic to the North. It has a total area of 20,131km2 (7,777sqm) and population of 11,058,300 [15].
The ethical clearance for the study was approved by the research ethics committee of Aminu Kano Teaching Hospital (AKTH) Kano and informed consent was also obtained from the participants (subjects).
This was a cross-sectional study of involving patients diagnosed with cirrhosis liver disease at the Department of Medicine, Aminu Kano Teaching Hospital (AKTH) between June, 2016 and December, 2016. The population study was a heterogeneous population consisting of different age group, ethnicities and educational status. Bio-data and other information of the patients were collected using informed consent forms with the assurance that all information obtained has to be treated with confidentiality.
A total of 37 blood samples were collected from patients diagnosed with cirrhosis liver disease attending Aminu Kano Teaching Hospital (AKTH) using blood collection vacutainer tubes and needles in vein puncture. This blood was then transferred into a plain container containing no anticoagulants for further use.
Gold Rapid Screen test with an enzyme-linked immunosorbent assay (ELISA) kits (Diagnostics Automation, Inc. California USA) that uses polystyrene micro well strips pre-coated with monoclonal antibodies specific to HBsAg was used in this study for the detection of Hepatitis B Surface Antigen (HBsAg) in the blood serum as described by Djebbi et al. (2009). The blood collected from suspected patients with Hepatitis B was left to clot and the serum was separated by centrifugation. The serum was then carefully withdrawn for testing. Using Pasteur pipette, 70-100µl (2-3 drops) of serum was added into the sample pad and observed for 15 minutes. The test has a sensitivity of 99.75% and specificity of 99.63%.
The hepatitis B disease was evaluated using liver enzyme tests by detecting the level of Alanine Amino-transferase (ALT), Aspartate Amino-transferase (AST), Alkaline Phosphatase (ALP), and liver function tests (LFTs) that include Direct Bilirubin (DB) and Total Bilirubin (TB) tests using kits as described by Changotra et al. [17].
3. Statistical Analysis
The T-test was performed for quantitative variables to check for statistical relationship between cirrhosis and HBV infection and the significant level for cirrhosis and HBV infection was set at probability level of P < 0.05
4. Results
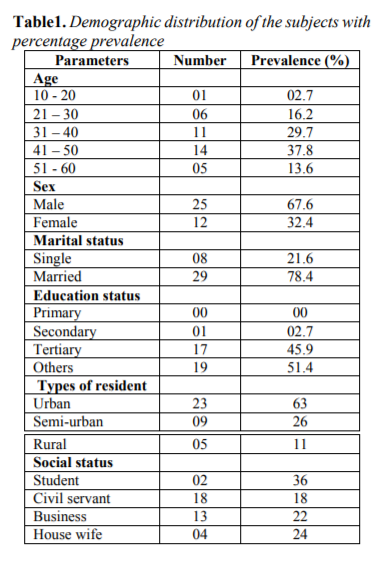
The Demographic distribution of the subjects is presented in Table 1. A total of 37 subjects participated in the study, all of which are patients diagnosed with cirrhosis liver disease. The age category, sex, marital status, educational status, social status and type of resident were considered for demographic distribution of the subjects.
Table 1
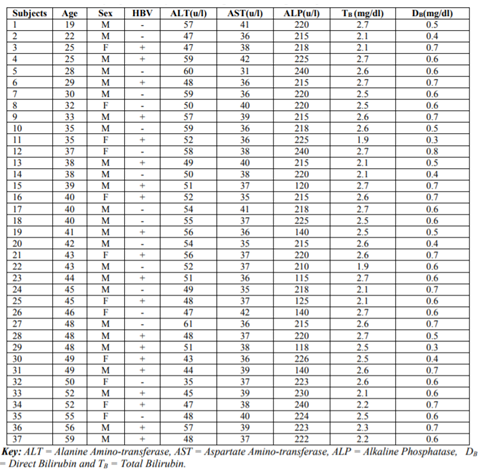
The hepatitis B infection was evaluated using Gold Rapid Screen test with an enzyme-linked immunosorbent assay (ELISA) kits while liver enzyme tests was conducted by detecting the level of Alanine Amino-transferase (ALT), Aspartate Amino-transferase (AST), Alkaline Phosphatase (ALP), and liver function tests (LFTs) by detecting Direct Bilirubin (DB) and Total Bilirubin (TB) tests. In the result, total of 20 subjects (54%) were found positive Hepatitis B virus out of 12 are males and 7 female subjects. Most of the values for ALT, AST, ALP, TB and TB are elevated above normal range.
Table2. Determination of hepatitis B infection among cirrhosis diagnosed patients
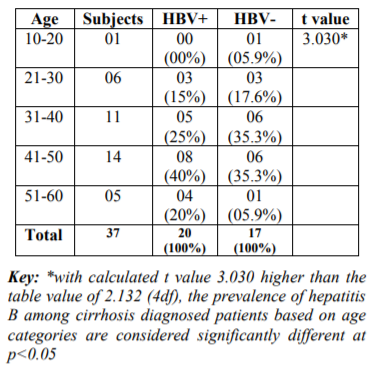
The prevalence of hepatitis B infection among cirrhosis diagnosed patients based on age group is presented in Table 3. The result showed that 20 out of 37 subjects have hepatitis B infections. Age category 41-50 years has the highest infection rate with 8 subjects (40%) while no subject is recorded among 10-20 years category.
Table3. Prevalence of hepatitis B virus among cirrhosis patients based on age categories
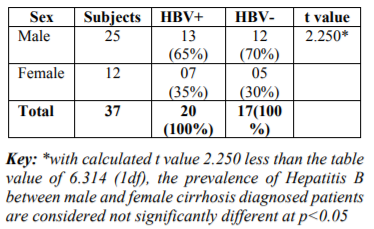
The prevalence of Hepatitis B virus with respect to sex among cirrhosis diagnosed patients is presented in Table 4. The result indicated that the hepatitis B infection is higher among male with total of 13 subjects which accounted for 65% than female with 7 subjects (35%).
Table4. Prevalence of hepatitis B virus among cirrhosis patients based on sex
5. Discussion
Liver cirrhosis is a common cause of morbidity and mortality worldwide and an important burden on the health care system. The present study was aimed to determine the prevalence of hepatitis B virus among patients diagnosed with liver cirrhosis disease in Kano, Northern Nigeria. In Nigeria, the prevalence of HBV infection has been found to be high and this places the country among the group of countries endemic for HBV infection [18]. Gabriel and Austin [19] reported that about 18 million Nigerians are currently infected with hepatitis B virus. Between 2000 and 2013, Musa et al. [20] obtained a pooled prevalence of 13.6% for adults and 11.5% for children from a study they conducted in Nigeria. Similarly, some investigators found a high HBV prevalence of 25.7% among blood donors [21], 23.4% among surgeons [22] and infants 16.3% [23].
Findings from the present study showed that hepatitis B virus is the most common cause of liver cirrhosis in Kano, Nigeria. The results indicated that 20 (54%) out of 37 cirrhosis diagnosed patients were infected with hepatitis B virus. Hepatitis B and C and alcohol consumption have been indicated as the main risk factors and probably contributing to the trend of the disease [24]. In this study, the values of liver enzymes are either maximum or above normal range which is clear indication of malfunction liver. Several studies were conducted on clinical evolution of liver cirrhosis. The result of this study was in conformity with that of Chang et al. [25]who found that chronic hepatitis B virus was the most common cause of liver cirrhosis in Singapore, accounting for almost two-thirds of the entire cohort (63.3%). Recently in a large secondary care hospital, Hsiang et al. [26] showed that the common primary etiologies for liver cirrhosis were chronic hepatitis B cirrhosis (37.3%), alcoholic liver disease cirrhosis (24.1%), chronic hepatitis C cirrhosis (22.3%) and non-alcoholic fatty liver disease cirrhosis (16.4%). Similar findings to the study were reported by some Asian countries such as Hong Kong, Taiwan and Malaysia where hepatitis B is the predominant etiology of liver cirrhosis [27,28,29].
The prevalence of hepatitis B infection among cirrhosis diagnosed patients based on age group showed that age category 41-50 years has the highest infection rate with total of 8 subjects (40%) while no subject is recorded among 10-20 years category. The age of the individual has been reported to be an influential risk factor in the development of diseases. Consistently, neonates and the elderly whose immune systems have been reported to be weak, enable the successful entry and establishment of most infections including hepatitis B virus. Old age, elevated alanine aminotransferase (ALT) levels and presence of HBeAg in the blood of individuals have been reported by McMahon [30] to be risk factors associated with the development of HBV infection. This finding supported the work of Adeniji and Anjorin in Ilori, Nigeria who found that majority of liver cirrhosis cases were found among the age category of 40 – 60 years old.
Male gender seems to be a risk factor for chronic liver disease. Several studies have reported male preponderance in liver cirrhosis [31]. In the present study, cirrhosis liver disease is higher among male with total of 25 subjects which accounted for 67% than female with 12 subjects i.e. 33%. This implies that the male to female ratio is 2:1. The present study also revealed that the hepatitis B infection is higher among male with total of 13 subjects which accounted for 65% than female with 7 subjects (35%). This finding correlates with that of Bundhamcharoen et al. [32]who reported that the prevalence cases in male 17,386 and in female of 12,241 (male: female ratio of 1.5:1).
6. Conclusion
Based on the finding of this study, the prevalence of hepatitis B infection among cirrhosis diagnosed patients based on age group showed that age category 41-50 years has the highest infection rate with total of 8 subjects (40%). The result also revealed that the hepatitis B infection is higher among male with total of 13 subjects which accounted for 65% than female with 7 subjects (35%). It is concluded that hepatitis B virus is one of the most common cause of liver cirrhosis.
References
- World-Health-Organization (WHO). Hepatitis B, Fact sheet No 204, updated 2015.
- Hadziyannis SJ. Review: hepatitis delta. J Gastroenterol Hepatol; 1997; 12: 289–98.
- Andrade ZA, Lesborders JL and Ravisse P. Fulminate hepatitis with microvescicular steatosis (a histological comparison of cases occurring in Brazil-Labrea hepatitis- and in central Africa-Bangui hepatitis). Rev. Soc. Bras.Med. Trop.1992; 25,155–160.
- Wedemeyer H. Re-emerging interest in hepatitis delta: new insights into the dynamic interplay between HBV and HDV. J Hepatol; 2010; 52:627–29.
- World-Health-Organization (WHO). Hepatitis Delta Virus. Global Alert and Response (GAR). http://www.who.int/csr/disease/hepatitis/whocd scs. 2011
- Benvegnu L, Gios M, Boccato S, Alberti A. Natural history of compensated viral cirrhosis: a prospective study on the incidence and hierachy of major complications. Gut 2004; 53:744-9.
- Hsiang JC, Bai WW, Raos Z, et al. Epidemiology, disease burden and outcomes of cirrhosis in a large secondary care hospital in South Auckland, New Zealand. Intern Med J. 2015; 45:160–169.
- Mokdad AA, Lopez AD, Shahraz S, et al. Liver cirrhosis mortality in 187 countries between 1980 and 2010: a systematic analysis. BMC Med. 2014; 18; 12(1):145.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012; 380:2197– 2223.
- Cristina S, Caterina S, Fabio V, Francesco C. Epidemiology of Liver Cirrhosis. Journal of Clinical and Experimental Hepatology. 2005; (5): 3 p272–272
- American Gastroenterological Association medical position statement: nonalcoholic fatty liver disease. Gastroenterology 2002; 123:1702-4.
- Dembele M, Maiga I, Minta D, Konate A, Diarra M, Sangare D et al. Study of antigen HBs and antivirus antibodies of hepatitis C during hepatopathies in Mali. Bull Soc Pathol Exot 2004; 97: 161-4
- Okeke EN, Malu AO, Obafunwa JO, Nwana EJ. Aetiological significance of alcohol in liver cirrhosis on the Jos Plateau. West Afr J Med 2002; 21: 12-4
- Intekhab A, Razaullah, Haider I, Humayun M, Taqweem MA, Muhammad N. Spectrum of Precipitating factors of Hepatic encephalopathy in liver cirrhosis. Pakistan J Med Res 2005; 44: 96-100
- National Population Commission (NPC). National population census result, 2006 Abuja Nigeria.
- Djebbi A, Rebai WK, Bahri O, Hogga N, Sadraoui A and Triki H . Serological markers, viral RNA and genotype of hepatitis delta virus in HBs antigen positive Tunisian patients. Pathol. Biol. 2009; 57,518–523.
- Changotra H, Dwivedi A, Nayyar AK and Sehajpal PK. Diagnosing different stages of Hepatitis B infection using a competitive polymerise chain reaction assay. Indian Journal of Medical Microbiology 2008; 26(2): 138-142.
- Henrietta OA, Maryam A. Seroprevalence of hepatitis B virus serological markers among pregnant Nigerian women.Annals of African Medicine. 2016; 15:20-27.
- Gabriel UPI, Austin OI. Seroepidemiology of hepatitis B surface antigenaemia among adult Nigerians with clinical features of liver diseases attending a primary-care clinic in a resource-constrained setting of Eastern Nigeria. North American Journal of Medical Sciences. 2013; 5:293–300.
- Musa BM, Bussell S, Borodo MM, Samaila AA, Femi OL. Prevalence of hepatitis B virus infection in Nigeria, 2000- 2013: A systematic review and meta-analysis. Nigerian Journal of Clinical Practice. 2015;18:163-172
- Bada AS, Olatunji PO, Adewuyi JO, Iseniyi JO, Onile BA. Hepatitis B surface antigenaemia in Ilorin, Kwara State, Nigeria. The Central African Journal of Medicine. 1996; 42:139-141.
- Belo AC. Prevalence of hepatitis B virus markers in surgeons in Lagos, Nigeria. East African Medical Journal. 2000;77: 283 -285
- Sadoh AE, Sadoh WE. Serological markers of hepatitis B infection in infants presenting for their first immunization. Nigerian Journal of Paediatrics. 2013; 40: 248-253.
- La Vecchia C, Levi F, Lucchini F, Franceschi S, Negri E. Worldwide patterns and trends in mortality from liver cirrhosis, 1955 to 1990. Ann Epidemiol1994; 4: 480-6.
- Chang, PE, Wong GW, James WQL, Lui HF, Chow WC, Tan CK. (2015) Epidemiology and Clinical Evolution of Liver Cirrhosis in Singapore. Annals Academy of Medicine. 2015; Vol. 44 6pp218-225
- Hsiang JC, Bai WW, Raos Z, et al. Epidemiology, disease burden and outcomes of cirrhosis in a large secondary care hospital in South Auckland, New Zealand. Intern Med J. 2015; 45:160–169.
- Fung KT, Fung J, Lai CL, Yuen MF. Etiologies of chronic liver diseases in Hong Kong. Eur J Gastroenterol Hepatol 2007; 19:659-64.
- Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. REVEAL-HBV Study Group. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology 2006; 130:678-86.
- Qua CS, Goh KL. Liver cirrhosis in Malaysia: peculiar epidemiology in a multiracial Asian country. J Gastroenterol Hepatol 2011; 26:1333-7.
- McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009; 49:45-55.
- Adeniji KA, Anjorin AS. Histopathological Assessment of the pattern of liver cirrhosis in a tropical population. Afr J Med Sci 2002; 31: 367-9
- National Center for Health Statistics. National Vital Statistics Report. Chronic liver disease/cirrhosis. Accessed April 17, 2007,
- Bundhamcharoen K, Teerawatananon Y, Vos T, Begg S. Burden of disease and injuries in Thailand. Nonthaburi: Bureau of Health Policy and Planning, Ministry of Public Health; 2004.