


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Bilateral Complete Duplicated Renal System and its Uncommon Presentation in a Young Female
Debansu Sarkar1,Pritesh Jain2,Dilip Kumar Pal3
2.Institute of Post Graduate Medical Education & Research, Kolkata-700020, India.
3.Professor& Head, Department of Urology, Institute of Post Graduate Medical Education & Research, Kolkata-700020, India.
Copyright :© 2017 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
A complete bilateral renal duplicated system can have various anatomical variations which lead to varied presentation. We are presenting a case of a young female who presented with continuous urinary incontinence since birth. On evaluation she was found to have bilateral complete renal duplicated system with right upper pole refluxing ectopic ureterocele opening at bladder neck and left upper pole ectopic ureter opening at urethrovaginal septum. She was treated with left upper pole nephrectomy with complete resolution of symptoms. Multifarious presentation of this congenital anomaly has dilemma not only in diagnosis but in decision making.
Female, Congenital abnormalities, Ureteral diseases, Urinary incontinence,Urology
1. Introduction
An incomplete duplex renal system is a common finding in general population with female predominance and is often asymptomatic. However complete renal duplication is an entity which due to aberrant insertion of ureter may lead to various complications with significant pathology, and often with long-term morbidity [1]. In a duplicated system according to Weigert-Meyer rule upper pole ureter insert inferolaterally and lower pole ureter superomedially which normally results in upper pole obstruction and lower pole reflux [2,3]. In our case right upper pole was dilated due to ectopic ureterocele and left upper pole was grossly dilated with ectopic insertion of ureter at urethrovaginal septum. Even with urinary incontinence from birth, female patients do not seek early treatment and often present at later age with complications. Variable presentation of a complete duplicated renal system as in our patient highlights diagnostic and therapeutic challenges in management of such cases.
2. Case Description
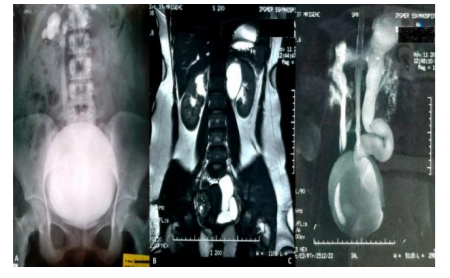
A 16-yrs old toilet trained female presented to us with complaints of urinary incontinence since birth. General Physical examination and local genitalia examination was unremarkable however dampening of clothes was present suggestive of some form of urinary leakage. Her routine blood investigations including complete blood counts and renal function tests were within normal limits. Urine analysis revealed plenty of pus cells whereas urine culture was sterile. Ultrasound of KUB (kidney ureter bladder) region revealed bilateral duplication of pelvicalyceal system and bilateral hydronephrosis. Ultrasound was also suggestive of dilated right ureter with uereterocele and dilated left ureter with possibility of ectopic insertion. Based on clinical history and ultrasound findings VCUG (Voiding cysto-urethrography) and MR urogram (Magnetic resonance urogram) was done. VCUG revealed Grade III VUR (Vesico-ureteral reflux) on right side [Figure 1A]. To further delineate anatomy MR urogram was done which revealed bilateral complete duplicated system with bilateral upper pole hydronephrosis. Upper moiety of right kidney was hydronephrotic with mild thinning of parenchyma, measuring 7mm in thickness; lower moiety was normal in morphology and signal intensity. Lower moiety ureter on both sides could be traced up to pelvis however exact site of insertion couldn’t be demonstrated. Upper moiety ureter on the right side is inserting ectopically in UB (Urinary bladder) just lateral to the vesicourethral junction. Upper moiety ureter on left side is grossly dilated and tortuous which was inserting below vesicourethral junction in the region of vagina with suggestion of obstruction of orifice. [Figure 1B, C].
Figure1B,C. MR urogram coronal and reconstructed images depicting bilateral complete duplex system with right upper pole dilated system due to ectopic ureterocele and left upper pole dilation due to obstructing ectopic ureteral insertion below vesicourethral junction near vagina.
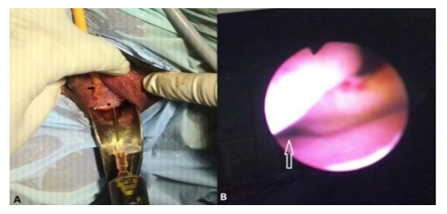
DTPA (Diethylene triamine pentaacetic acid) renogram was done to evaluate function, which revealed GFR of 40.38 ml/min and 43.78 ml/min of left and right kidney respectively. Left upper moiety function was minimal. On evaluation under anaesthesia vaginal speculum examination revealed indentation of hugely dilated left upper moiety ureter inside vagina [Figure 2A]. Cystourethrscopy revealed normal insertion of bilateral lower moiety ureter. Right upper moiety ureter was inserting as ectopic ureterocele near urinary bladder neck [Figure 2B]. Even after thorough inspection left upper moiety ureter insertion couldn’t be identified. Under USG guidance left upper moiety puncture was done and methylene blue dye injected but leakage of dye couldn’t be appreciated. Through vagina dilated ureter was punctured and povidone-iodine injected which revealed leakage of urine on anterior aspect of urethrovaginal septum [Figure2A].
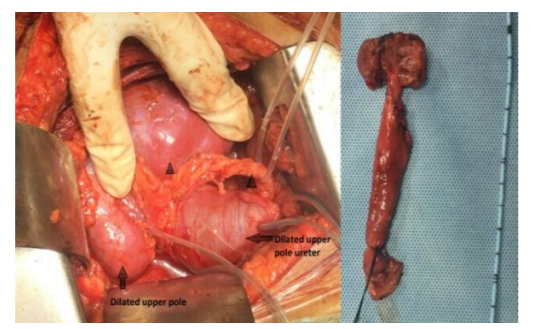
After identification of ectopic insertion of left upper moiety ureter, left upper pole nephrectomy was done. Intraoperatively left side upper moiety was found small and hydronephrotic with hugely dilated ureter [Figure 3]. Patient’s recovery was uneventful with complete resolution of symptoms at one month follow-up. For right upper pole VUR she was advised regular follow-up.
3. Discussion
Incidence of duplex kidneys has been seen in less than 1 % of general population. [1] Bilateral duplex system is found in approximately 17- 33 % cases with female predominance. [4] Embryologically Complete duplication is usually from two ureteral buds stimulating two metanephric mesenchymes whereas splitting of ureteral bud leads to incomplete duplication. [5] Clinical significance of these anomalies relies on the location of the buds and their interplay with the developing kidney. According to Weigert-Meyer rule, the future lower pole ureter separates from Wolffian duct earlier and thus migrates superiorly and laterally as the urogenital sinus grows. It further states that upper pole ureter usually leads to obstruction and lower results in refluxing however exceptions have been reported [2,3]. In our case also right upper pole ureter was refluxing because of ectopic ureterocele formation. An ectopic ureterocele includes those in which some portion of the ureterocele is situated permanently at the bladder neck or urethra [6]. Though there is great variability in the presentation of either ectopic ureter or ureterocele, there are several patterns that may be anticipated.
Clinically patients may be asymptomatic or have discrete presentation like fever, flank pain, acute or recurrent urinary tract infection, failure to thrive, abdominal mass, unilateral or bilateral hydronephrosis, bladder outlet obstruction, vaginal discharge, inter-labial mass etc. Urinary incontinence in toilet trained females is a common presentation of ectopic ureter. Male may present with epididymo-orchitis, painful ejaculation or lower urinary tract symptoms etc.
Antenatal ultrasound has dramatically increased detection of significant urinary tract anomalies which help in providing appropriate treatment and minimise long term complication. Postnatal patients with duplex system represent no more than radiologic curiosities. Various radiological imaging has been used in evaluation of such cases like Ultrasound, IVU (Intravenous urogram), VCUG, CT urogram, MR urogram and Radionuclide renal imaging. The ultrasound image will usually provide the anatomic diagnosis and permit inference of functional assessment. IVU may not clearly demonstrate anatomy in poorly functioning system. VCUG provides the most emphatic evaluation of the bladder, ureter and urethra in ureterocele and ectopic ureter, and is an obligatory imaging test. Presence of reflux has an important role in decision making. MR urogram can provide the most detailed images of an affected urinary tract, as a whole with functional information and also useful in detection of associated anomalies. Such conditions might initially go undetected during imaging as the affected renal moiety may not be dilated, and the level of suspicion must be guided by a careful history and occasionally physical examination. Cystourethroscopy and vaginoscopy should take note of the character of the urethra, bladder neck, and trigone relative to the ureterocele or ectopic ureter. In our case direct puncture of ureter indentation in vagina and instillation of povidone-iodine helped us to identify ectopic ureter opening. This manoeuvre can be used to identify ectopic ureter opening when other methods fails to localise insertion of ectopic ureter.
Goals of therapy in such cases should be clearly defined and factored into the clinical decisions. Preservation of renal function, maintenance of urinary continence, elimination of infection, obstruction, and reflux are priority of the therapy. Functional urinary assessment in association with an ectopic ureter or ureterocele is the foundation for both initial management and postoperative care, and this is usually best afforded by dimercaptosuccinic acid (DMSA) imaging. The natural history of VUR in association with duplicated systems is not completely clear however based on available data a trial of antibiotics and careful observation can be given in low grade reflux. For ectopic ureter decision is much clearer than ureterocele and largely defined by affected moiety function and presence of reflux in other moiety. In our case left upper pole nephrectomy was done as upper pole was poorly functioning. Various surgical treatments are described for ureterocele depending on several factors, including presenting symptoms, ectopic versus orthotopic position, presence or absence of reflux, and function of the associated upper-pole moiety [7]. Treatment includes transurethral incision, upper pole nephrectomy, ureteroureterostomy, ureteropyelostomy ureterocele excision and Common-Sheath Reimplantation etc [8].
4. Conclusion
Bilateral complete renal duplicated system is a rare congenital abnormality with discrete presentation. These cases due to various anatomical rearrangements and clinical presentation pose difficulty not only in diagnosis but also in treatment as highlighted in our case.
References
- S. M. Whitten and D. T. Wilcox, “Duplex systems,” Prenatal Diagnosis. 2001;21(11):952–57.
- C. Weigert: Über einige Bildungsfehler der Ureteren. Virchows Archiv für pathologische Anatomie und Physiologie und für klinische Medizin, Berlin, 1877, 70: 490.
- R.Meyer:ZurAnatomieund Entwicklungsgeschichte Der Ureterverdoppelung. Virchows Archiv für pathologische Anatomie und Physiologie und für klinische Medizin, Berlin, 1907, 87: 408.
- W. E. Kaplan, P. Nasrallah, and L. R. King, “Reflux in complete duplication in children,” The Journal of Urology. 1978; 120:220-22.
- Dahnert W. Radiology Review Manual. 5. Philadelphia, PA: Lippincott Williams and] Wilkins; 2003. Urogenital tract; 977–78.
- Glassberg KI, Braren V, et al. Suggested terminology for duplex systems, ectopic ureters and ureteroceles. J Urol 1984;132(6):1153–54.
- Controversies in the management of ectopic ureteroceles. Coplen DE, Barthold JS Urology. 2000 Oct 1; 56(4):665-68
- Craig A. Peters, MD, and Cathy Mendelson Ectopic Ureter, Ureterocele, and Ureteral Anomalies In: Wein JA. Campbell-Walsh Urology. 11th ed. Philadelphia: Saunders Elsevier 2016: 3096-97.