


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Atypia of Undetermined Significance in Thyroid Fine-Needle Aspiration Cytology: An Institutional Experience
Direnc Yigit1*, Mehmet Ilker Turan2, Mehmet Celik3, Ahmet Nezihi Oygur4, Cumhur Arici5
2.Antalya Kepez State Hospital, Department of General Surgery, Antalya, Turkey
3.Antalya Kepez State Hospital, Department of Endocrinology and Metabolism, Antalya, Turkey
4.Olimpos Hospital, Department of General Surgery, Antalya, Turkey
5.Akdeniz University Faculty of Medicine, Department of General Surgery, Antalya, Turkey
Copyright :© 2019 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Aim: Thyroid nodules have % 3-7 frequency in general population. FNA biopsy is an important diagnostic tool for patients with thyroid nodules. There are many reporting systems for FNA biopsy and Bethesda system is the most common one. The aim of this retrospective study is to detect the atypia with undetermined significance rates in the patients who has been performed FNA biopsy and to evaluate the concomitant biopsy results of these patients and to evaluate the types of operation and malignancy rates who has been performed surgical operation.
Materials and Methods: In this study 3371 patients who underwent thyroid FNAB between 2010 January and 2016 July in Akdeniz University Hospital were evaluated retrospectively and 61 patients who have undergone total thyroidectomy or thyroid lobectomy were enrolled in the study.
Results: The frequency of atypia with undetermined significance was found as 8%. When FNAB and final pathology results were evaluate together, first FNAB’s sensitivity was found as 100% and specificity was %5. The first FNAB’s positive predictive value was 30% and negative predictive value was 100%. The sensitivity and specificity of second FNAB procedures, which have been performed in patients whose first FNAB cytologic examination revealed AUS, were 75% and 0%, respectively. There were no statistically significant differences between first and second FNAB’s malignancy ratios in this study.
Conclusion: The frequency of atypia with undetermined significance in patient series in the literature is between 3-10% and in our study; we found this rate as 8%. The malignancy rates according to final patology reports are between 22-35% and we found this rate as 29,5%. However, there are contradictory data for surgery decision according to first and second FNAB’s malignancy ratios, and further studies with larger patient series are required.
Thyroid nodules, Bethesda system, Atypia with undetermined significance,Surgery
1. Introduction
Thyroid nodules are seen in the general population at a frequency of 3-7% [1,2]. The most widely used reporting system in the pathology of thyroid nodule fine needle aspiration biopsy (FNAB) is Bethesda.
According to Bethesda classification, cytological diagnosis is divided into six groups. These are; nondiagnostic, benign, atypia of undetermined significance (AUS)/ follicular lesion of undetermined significance (FLUS), follicular neoplasm/suspicious for follicular neoplasm (FN), suspicious for malignancy, and malignant. Among these, 3-18% of all FNAB’s results are observed AUS [3-6]. It is recommended to re-administer FNAB with USG after 3-6 months in this group according to the ATA guideline. Importance of recurrent FNAB In patients with AUS or a category with higher risk of malignancy, surgery is recommended. The nature of the surgical procedure is controversial. While some centers prefer total thyroidectomy, some centers recommend lobectomy and intra-frozen examination on the side where atypia is detected [7]. The aim of this study was to determine the rates of uncertain atypia in the patients who underwent FNAB due to thyroid nodules, to evaluate the results of FNAB applied in these patients, to determine the operation type, to determine the malignancy rates and to compare the results with the literature.
2. Materials And Methods
In this study, 3371 patients with FNAB were evaluated retrospectively and 270 patients who had atypical results were determined. In this study, 3371 patients who underwent FNAB between January 2010 and July 2016 were evaluated retrospectively. 61 patients who underwent a first FNAB or FNAB results for 3-6 months were included in the study. The demographic data of the patients and FNAB results were recorded from the patient files. As a result of the first FNAB, 25 of the patients were operated and 103 were followed with routine Endocrine out patientclinic control. The second FNAB was performed in 142 patients at least 3 months later. According to the results of the second FNAB, 28 patients were operated. Eighty three patients were followed and 31 patients underwent the third FNAB. As a result of the third FNAB, 7 of the patients were operated. While 17 patients were being followed up, 9 patients underwent repeat biopsy with the need for a fourth FNAB. Only one of the patients who underwent the fourth FNAB was operated and 8 of the patients underwent medical follow-up. Statistical analysis of the data of the patients was performed using SPSS v20 (IBM) program. The data obtained in the study were evaluated by means of mean, standard deviation, chi-square test, difference test between independent samples and sensitivity and specificity analyzes. The data were analyzed according to 95% confidence interval and p values less than 0.05 were considered significant.
3. Results
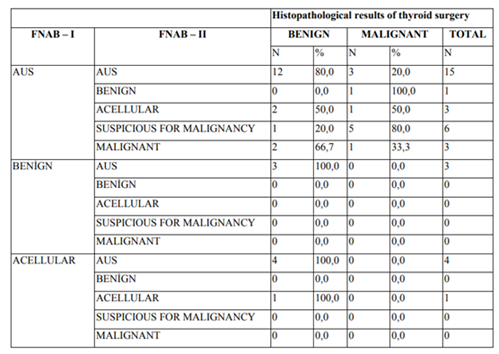
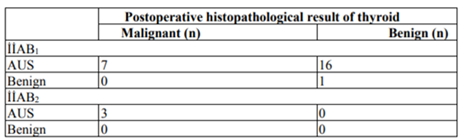
Of the patients included in the study, 24.6% (n = 15) were male and 75.4% (n = 46) were female and the male to female ratio was approximately 1:3. The mean age was 50.9 ± 11.69 (min: 27, max: 74) in the study group. The mean age was 52.50 ± 11.27 for males and 50.50 ± 11.92 for males. There was no statistically significant difference between the genders in terms of age distributions (p = 0.887). Total thyroidectomy was performed in 77% (n = 47) of the patients, 11.5% (n = 7) of left thyroid lobectomy and 11.5% (n = 7) right thyroid lobectomy was performed. Thyroid nodule FNAB was performed in 3371 patients with atypia in 270 patients and the rate of hast AUS hast was 8% in our study. Thyroid nodule was performed in 28 patients who were diagnosed as AUS as a result of FNAB cytology. The results of FNAB for the second time were reported as 15 patients with AUS, 1 with benign, 3 with a cellular cytology, 6 with suspicious for malignancy and 3 with malignant. In the postoperative histopathology of 15 patients with AUS cytology twice in a row; It was determined that 80% of the patients were benign (n = 12) and 20% (n = 3) were malignant (Table-1). Total thyroidectomy was performed in a patient who had first thyroid nodule FNAB cytology was AUS and a second FNAB cytology was benign. The histopathological result of this patient was found to be malignant. The first FNAB cytology atypia and the second FNAB cytology were reported as suspicious for malignancyin the histopathological examination of the surgical materials of 6 patients, in 20% (n = 1) benign and 80% (n = 5) malignant results were reported. In the histopathological examination of the first FNAB cytology atypia and the malignant specimens of the second FNA cytology, 66.7% (n = 2) of the patients had benign and 33.3% (n = 1) had a malignant result. The pathological examination of the operation materials of the patients who underwent FNAB because of nodular thyroid pathology and then underwent surgery was 29.5% (n = 18) and 70.5% (n: 43) were reported as benign. Sensitivity and specificity of the first FNAB cytology were 100% and 5%, respectively. Based on this result, 100% of malignancy cases could be detected with the first FNAB, whereas only 5% of cases with benign etiology could be classified as benign. The positive diagnostic value of the first FNAB was 30% and the negative diagnostic value was 100%. In the light of these data, the first FNAB cytology revealed 30% of patients who were given AUS as a result of malignancy. Postoperative histopathological results were benign in 100% of the patients who had benign cytology at the first FNAB. As a result of the pathological examination of the surgical materials of the patients with atypia at the first FNAB, 38.8% (n = 7) were reported as malignant and 61.2% (n = 18) were reported as benign. The postoperative histopathological evaluation of the cases reported to be AUS after the cytological examination in the second time was 44% malignant and 56% was a benign result (table 1, table 2). When postoperative histopathological results were evaluated, no statistically significant difference was observed between the postoperative findings of patients who had undergone FNAB once or twice (P = 0.830). The incidence of malignancy under 50 years of age was 38% (n = 8), and 45% (n = 10) of the patients in the ≥50 age group.
4. Discussion
Thyroid nodules are common in adults with a prevalence of 4-7% [2]. The main purpose of the approach to the nodules detected in the thyroid gland is to avoid unnecessary surgical interventions. Diagnostic results of FNAB, a cheap and reliable method for cytological examination of specimens taken from thyroid nodules, may provide more precise findings [8-10]. In the literature, there are studies reporting AUS in 4 -15% of the thyroid nodules after FNAB [11]. The AUS / FLUS categories reported by the Bethesda system show a 5-15% malignancy risk [12]. According to the Bethesda system, the incidence of AUS / FLUS is lower than 7%, but a very heterogeneous distribution can be observed depending on the center of the procedure [13,14]. In our study, this rate was 8% in accordance with the literature. In a meta-analysis study of 51 publications from 2009 to 2014 with the evaluation of 145920 FNAB cytology, the incidence of malignancy was found to be 23-31% by the evaluation of thyroidectomy materials in patients reported as AUS [15]. In the literature, it has been reported that the incidence of postoperative malignancy in patients with thyroid nodule FNAB cytology AUS may vary between 6-48% [14,16-19]. In our study, this rate was found to be 29.5% in accordance with the literature. In their study, Shrestha et al. reported 26% malignancy in the final pathology after the patients who were first diagnosed as FNAB cytology AUS and evaluated with clinical risk factors. In the same study, the rate of malignancy reported in the final pathology was 15% in patients who underwent surgery after recurrent FNAB cytology [14]. Seo et al., evaluate the risk of malignancy of thyroid nodules, age (≥45), female gender, the maximum diameter of the nodule is less than 1.5 cm, the presence of more than two ultrasonographic criteria and the results of two or more FNAB cytology AUS reported a one-way analysis of the reporting parameters. In this study, they reported that reporting of AUS results in two or more recurrent FNAB cytology increased the likelihood of malignancy detection [20]. In our study, the rates of malignancy after the first FNAB and after repeated FNAB were found to be 38% and 44%, respectively. However, there was no statistically significant difference in the incidence of postoperative malignancy of thyroid between the patients who underwent an initial biopsy and recurrent biopsy (p = 0.83). We found that 56% of the patients had benign pathology even after recurrent FNAB. In our study, we found that the risk of malignancy in thyroid nodules did not significantly increase with age. Similar to our findings in the literature, there are also reports indicating that age is not effective on the development of malignancy in thyroid nodules. Kwang et al. Reported that age is not a factor that affects the risk of malignancy as a result of a multidimensional analysis of the malignancy risks of patients with the first FNAB cytology AUS [21]. In the study conducted by Seo et al, it has been shown that being over 45 years of age has no effect on the malignancy of thyroid nodule [20].
5. Conclusion
In patients who are multidisciplinary evaluated by general surgery, endocrinology and radiology departments, surgery may be suggested even if cytologic examination of first FNAB of thyroid nodule reveals AUS.
References
- Tunbridge, W.M., Evered, D. C., Hall, R. ve ark. The spectrum of thyroid disease in a community: the Whickham survey. Clin Endocrinol (Oxf), 1977. 7(6): 481-93.
- Ezzat, S., Sarti, D. A. Cain, D. R.ve ark., Thyroid incidentalomas. Prevalence by palpation and ultrasonography. Arch Intern Med, 1994. 154(16): 1838-40.
- Nayar, R. ve M. Ivanovic, The indeterminate thyroid fine-needle aspiration: experience from an academic center using terminology similar to that proposed in the 2007 National Cancer Institute
- Renshaw, A.A., Accuracy of thyroid fine-needle aspiration using receiver operator characteristic curves. Am J Clin Pathol, 2001. 116(4): 477-82.
- Yang, J., Schnadig, V., Logrono, R. ve ark., Fine-needle aspiration of thyroid nodules: a study of 4703 patients with histologic and clinical correlations. Cancer, 2007. 111(5): 306-15.
- Yassa, L., Cibas, E., S. Benson, C. B. ve ark., Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer, 2007. 111(6): 508-16.
- Prades, J.M., Querat, C., Dumollard, J. M. ve ark., Thyroid nodule surgery: predictive diagnostic value of fine-needle aspiration cytology and frozen section. Eur Ann Otorhinolaryngol Head Neck Dis, 2013. 130(4): 195-9.
- Jo V.Y., Stelow, E. B., Dustin, S. M. ve ark., Malignancy risk for fine-needle aspiration of thyroid lesions according to the Bethesda System for Reporting Thyroid Cytopathology. Am J Clin Pathol, 2010. 134(3): 450-6.
- Mazzaferri, E.L., Management of a solitary thyroid nodule. N Engl J Med, 1993. 328(8): 553-9.
- Kaynaroğlu V., Tiroid ve paratiroid, Tiroid Nodüllerine Genel Yaklaşım, Temel Cerrahi., Sayek İ., Editor. 1996, Güneş Kitabevi,:Ankara. 176-192.
- Bonzanini M., Amadori, P., Morelli, L.ve ark., Subclassification of the "grey zone" of thyroid cytology; a retrospective descriptive study with clinical, cytological, and histological correlation. J Thyroid Res, 2011. 2011: 251-680.
- Wong L.Q., LiVolsi V.A., ve Baloch Z.W., Diagnosis of atypia/follicular lesion of undetermined significance: An institutional experience. Cytojournal, 2014. 11: 23.
- Haugen B.R., Alexander, E. K., Bible, K. C.ve ark., 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid, 2016. 26(1): 1-133.
- Shrestha R.T. ve Hennessey J.V., Cytologic subclassification of atypia of undetermined significance may predict thyroid nodules more likely to be malignant at surgery. Diagn Cytopathol, 2016. 44(6): 492-8.
- Straccia P., Rossi E. D., Bizzarro T.ve ark., A meta-analytic review of the Bethesda System for Reporting Thyroid Cytopathology: Has the rate of malignancy in indeterminate lesions been underestimated? Cancer Cytopathol, 2015. 123(12): 713-22.
- Ohori N.P. ve K.E. Schoedel, Variability in the atypia of undetermined significance/follicular lesion of undetermined significance diagnosis in the Bethesda System for Reporting Thyroid Cytopathology: sources and recommendations. Acta Cytol, 2011. 55(6): 492-8.
- VanderLaan P.A., Marqusee E., and Krane J.F., Clinical outcome for atypia of undetermined significance in thyroid fine-needle aspirations: should repeated fna be the preferred initial approach? Am J Clin Pathol, 2011. 135(5): 770-5.
- Ho A.S., Sarti E. E. Jain K. S.ve ark., Malignancy rate in thyroid nodules classified as Bethesda category III (AUS/FLUS). Thyroid, 2014. 24(5): 832-9.
- Mathur A., Najafian A. Schneider E.B.ve ark., Malignancy risk and reproducibility associated with atypia of undetermined significance on thyroid cytology. Surgery, 2014. 156(6): 1471-6; 1476.
- Seo J.W., Jang, A.L., Suh S. H. ve ark., Atypia of undetermined significance on thyroid fine needle aspiration - risk factors for malignancy. Clin Otolaryngol, 2016.
- Lee K.H., Shin, J.H., Oh Y. L. ve ark., Atypia of undetermined significance in thyroid fine-needle aspiration cytology: prediction of malignancy by US and comparison of methods for further management. Ann Surg Oncol, 2014. 21(7): 2326-31.