


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Textiloma Resembling Abdominal Tumor
Luis Angel Medina Andrade1*, Carlos Eduardo Rodriguez Rodriguez2, Pedro Leonardo Villanueva Solorzano2, Alberto Robles Mendez Hernandez2, Araceli Esteban Chaparro3, Brigitte Marlene Chevillon Castillo4, Sergio Ruben Cobo Ovando4, Maria Veronica Jordan Lopez4
2.General Surgery Resident, Universidad La Salle, Hospital Angeles Metropolitano, Mexico City, Mexico
3.Medical Student, Hospital General de México, Mexico City, Mexico
4.Medical Student, Hospital General Regional 17, IMSS, Cancún, Mexico
Copyright :© 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: Textiloma is a known complication of surgical procedures, even scheduled, and symptoms of chronic abdominal pain after surgery not related with the procedure must alert us about this possibility.
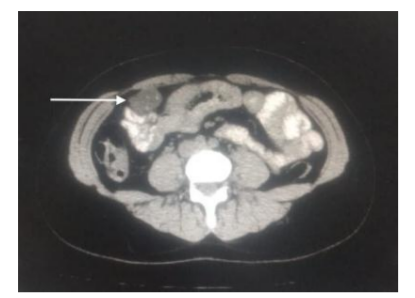
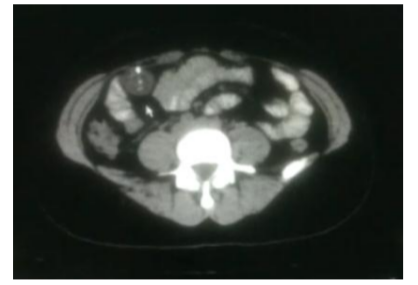
Case: Female patient of 35 years-old presents to follow up in general surgery consult two months after elective laparoscopic cholecystectomy without complications apparently, referring abdominal pain of low intensity in right lower quadrant. At physical exam without any identifiable abnormality. For location an inguinal hernia was suspected but ultrasound discard this. Was treated with analgesics without improvement. A CT scan reveals a right rectum muscle tumor and patient was scheduled for a laparoscopic exploration for the surgical background. During surgery an encapsulated fragment of the bag to extract gallbladder and many biliary stones inside was found, and an extraction complete without complications.
Conclusion: Many measures along the surgical technique have been developed to avoid accidental complications like textiloma, with subsequent increased morbidity, but in this case they are not useful, only attention during surgical procedure could avoid such complication.
Tumor like, Textiloma, Cholecistectomy complications, Abdominal tumor,Surgery
The textiloma or gossypboma is defined as a foreign body left behind during an operation. The incidence is not well estimated secondary to misdiagnosis or abscense of reports about it, by the medico-legal implications, but some previous articles report it between 1 in 1000 cases and 1 in 10000 cases. The presentation varies from asymptomatic to abdominal pain and serious complications like intestinal perforation, and the time of presentation could be from days to years after surgery, for this reason the diagnosis sometimes is difficult[1].
2. Case Report
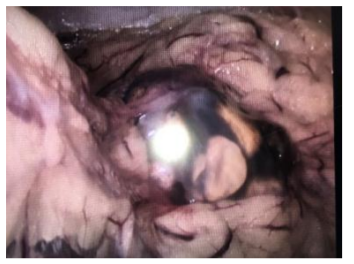
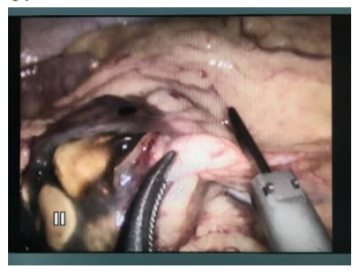
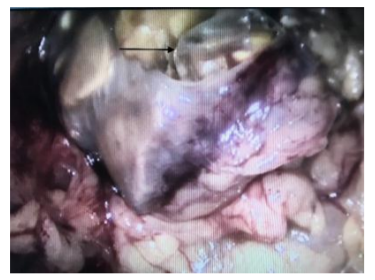
Female patient of 35 years-old presents to follow up in general surgery consult two months after elective laparoscopic cholecystectomy without complications apparently, referring abdominal pain of low intensity in right lower quadrant. At physical exam without any identifiable abnormality, but referring occasional sporadic pain of low intensity near inguinal region, it was controlled with standard analgesics, but each time was more frequent. For the referred location an inguinal hernia was suspected an ultrasound discard this possibility. During time of study in the consult was treated with analgesics without improvement. A CT scan reveals a right rectum muscle dependent tumor and patient was scheduled for a laparoscopic exploration for the surgical background and possibility of a related lesion more than the referred tumor by the radiologist (Fig. 1 and 2). During surgery an encapsulated tumor was observed in the right lower quadrant (Fig. 3), after dissection with ultrasonic device a fragment of the bag to extract gallbladder, and many biliary stones inside was found (Fig 4 and 5), and an extraction complete without complications. Patients was discharged the same day and after 2 months of follow up she remains asymptomatic.
3. Discussion
The textiloma or gossypiboma is refered to foreign bodyes such as cotton, gauze or other surgical materials left behind during operations. The incidence is very variable and is not reliable by the great number of cases without any report by the legal consequences of this[1-3].
It has been reported that some risk factors for the occurrence of those accidents are the surgical emergencies, change of surgical team during the operations, absence of material quantification before surgical incision and previous to closure, surgeries late in the night, long surgeries, change of surgical technique. Other reports mention that only 30% of textilomas are presented in emergency surgeries and 70% in elective[1].
This complication is observed in all specialities but the more frequent are general surgery (52%), gynecologic (22%), urologic/vascular (10%), and orthopedic/spinal surgery (6%)[1].
The symptoms associated with textilomas are extremely variable, ranging from asymptomatic cases for over 35 years to abdominal pain right after surgery, intestinal obstruction, fistula formation, granulomas, tumor like lesions, abscesses, fever, biliary obstruction and chronic pain[2-4].
The diagnosis sometimes is difficult by the high degree of suspicion required. The first phase for the diagnosis is the x-ray study, confirming the presence of gauze material in 90% of the cases and being the more frequent material left behind, but in some cases this test is negative and in the other 10% the material has not a radiopaque component to identify. Some materials without this marks are plastic materials, bags, mesh or diverse surgical components[2]. If the x-ray is not conclusive other imagine studies like ultrasound, CT scan or MRI are needed.
Once the foreign body is left behind two kinds of reactions are observed: an exudative tissue reaction leading to acute abscess formation or an aseptic fibrous tissue reaction which involves slow adhesions formation, such as granulomas or encapsulation, this last is the one observed in tumor like lesions and could be asymptomatic for years after surgery[5,6]. The tumor like lesions are specially difficult to distinguish from a textiloma only because some of them share some imaging characteristics in CT scans or ultrasound[5,6].
When this tumor like lesions are observed like in the presented case, one option is to practice an ultrasound guided biopsy, but the one most used is a surgical exploration with remotion of the lesion and send it to pathology exam if their origin is not obvious.
In this cases the acute presentation is associated with complications and mortality between 8-40% in some reports[4], so the possibility must be commented to the patients, and in case of confirmation, a good communication between the surgical team and patient’s family is crucial for a good outcome.
4. Conclusion
Many safe points have been developed in the operating room to avoid complications like a wrong site of incision, incorrect surgery or textilomas. In the presented case our theory was a bag rupture during extraction that was not perceived by the surgical team, leaving behind a fragment of the bag with some biliary stones inside, with the subsequent encapsulation by the mesentery. All the surgeries must complete the stablished systematized for the safety of the patients and avoid complications, with all the surgical team being responsible for any neglect.
References
- NORIYUKI YAMAMURA, KIYOKAZU NAKAJIMA, TSUYOSHI TAKAHASHI, MAMORU UEMURA, et. al. Intra-Abdominal Textiloma. A Retained Surgical Sponge Mimicking a Gastric Gastrointestinal Stromal Tumor: Report of a Case. Surg Today (2008) 38:552–554.
- Gaspar Alberto Motta Ramírez, Oliva González Burgos, J osé Arturo Castillo Lima, Evaristo Villalobos García, Material quirúrgico olvidado: Gossypiboma, textiloma, gasoma. Anales de Radiología México 2007;4:285-296.
- Bayindir Cimsit, M. Keskin, I. Ozden, and A. Alper, Obstructive jaundice due to a textiloma mimicking a common bile duct Stone. J Hepatobiliary Pancreat Surg (2006) 13:172–173.
- Víctor Huggo Córdova-Pluma,César Augusto Vega-López, Federico Armando Castillo-González, Gilberto Bernabé Cornejo-López. Textiloma abdominal: reporte de caso. Med Int Mex 2012;28(4):398-402.
- Koray Agras, Ege Can Serefoglu, Engin Duran, Mesut Gurdal, Retroperitoneal textiloma mimicking a renal tumor: Case Report. Int Urol Nephrol (2007) 39:401–403.
- B. B. Dash, R. Mahey, A. Kriplani, N. Agarwal, Neerja Bhatla. Textiloma, a rare pelvic tumor. Arch Gynecol Obstet (2010) 282:707–709.