


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Laparoscopic Appendectomy as Main Therapeutic Option of Appendicitis
Ming-Ho Wu1*,Han-Yun Wu1
Copyright :© 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Objective: To understand the frequency of laparoscopic appendectomy (LA) for appendicitis and to analyze the diagnostic discrepancies among the radiologist, surgeon, and pathologist in a regional hospital.
Patients and Methods: There were 400 patients who underwent appendectomy during a two-year period of 2015 and 2016. The ratio of LA comparing to open appendectomy (OA) was counted. The interval between occurrence of symptom and operation, clinical diagnosis, laboratory data, report of computed tomography will be justified by pathologic finding. Management of post-operative complications was also reviewed.
Statistical Analysis: Statistical analysis was performed using the Statistical Package for Social Sciences (IBM SPSS Statistics 22). A P-value less than 0.05 is considered as significant.
Results: Of 400 patients with suggestive of appendicitis, 388 (97%) underwent LA and 12 (3%) OA. Among them, 265 (66.3%) were diagnosed as non-perforated appendicitis, 75 (18.8%) perforated appendicitis, 57 (14.2%) mild or non-inflammation of appendix, and 3 (0.7%) malignancy of appendix. Operative complications occurred in 11 (2.7%) patients. Discrepancies between the laparoscopic findings with pathologic reports were in 37 (9.3%) patients. Of 194 patients taking computed tomography, 19 (9.8%) were not compatible between CT reports and pathologic findings.
Conclusion: LA was the main therapeutic option of appendicitis. Early surgery of appendicitis could reduce postoperative complication.
Laparoscopic Appendectomy; Open Appendectomy; Appendicitis,Surgery
Laparoscopic appendectomy (LA) has been recognized as a standard procedure in the treatment of appendicitis because the procedure was associated with a shorter hospital stay and lower incidence of wound infection [1-4]. LA rate significantly increased in United State [5]. Minimally invasive surgery is the golden surgical training of Show Chwan Medical Care Corporation. As one hospital of the corporation, we always consider the minimally invasive procedure used in all surgical patients. Hence, LA is the basic skills in the Division of General Surgery that need to have self quality control.
2. Patients And Methods
The institutional review board of Show Chwan Memorial Hospital approved this study and granted a waiver of the informed consent process (SCMH IRB No.1060705). There were 400 patients who underwent appendectomy during a two-year period of 2015 and 2016 in the regional hospital. The rate of LA was counted. The interval between occurrence of symptom and operation, clinical diagnosis, reports of computer tomography, operation time, hospital stay, and grade of appendicitis were studied. Patients with postoperative complications were also reviewed. Discrepancies among surgeon, radiologist, and pathologist were also collected for analysis.
All these patients presented to the Emergency Department with abdominal pain suggestive of appendicitis. The studies included history taking, physical examination, laboratory tests of blood and urine, X-ray of chest film and abdomen. Computed tomography of abdomen was reserved for undetermined acute abdomen.
LA using 3 ports was the first choice to treat the appendicitis. OA was performed using traditional Grid –Iron incision over the Mc-Burney’s point. In case of perforated appendicitis, a Jackson-Pratt drain was used for drainage.
Data were tested for normality, and presented as mean and standard error. Categorical data were presented as frequencies and percentage and compared by the Chi-square test. Parametric and nonparametric continuous data were presented as mean and standard deviation and evaluated by the Student’s t test and Mann–Whitney U test respectively. A P-value less than 0.05 was considered as significant. Statistical analysis was performed using the Statistical Package for Social Sciences (IBM SPSS Statistics 22).
3. Results
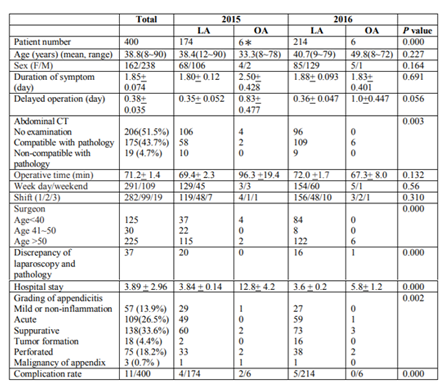
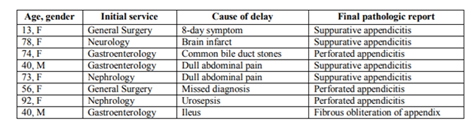
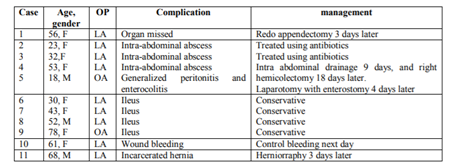
Of 400 patients with suggestive of appendicitis, 388 (97%) underwent LA, and 12 (3%), including one conversion to OA. Among them, 265 (66.3%) were diagnosed as non-perforated appendicitis, 75 (18.8%) perforated appendicitis, 57 (14.2%) mild or non-inflammation of appendix, and 3 (0.7%) malignancy of appendix. The aforementioned 265 non-perforated appendicitis consisted of 109 acute appendicitis, 138 suppurative appendicitis, and 18 tumor formation of appendicitis. The aforementioned 57 mild or non-inflammation of appendix consisted of lymphoid hyperplasia (n=25), fecal impaction (n=19), periappendicitis (n=5), mild appendicitis (n=3), normal appendix (n=2), fibrous obliteration (n=1), eosinophilic appendicitis (n=1), and chronic appendicitis (n=1). Three patients with appendiceal malignancy included carcinoid, adenocarcinoma, and low grade mucinous neoplasm. Of all patients, 277 (69.3%) underwent appendectomy on the day of admission, 109 (27.3%) the next day, 6 (1.5%) 2 days, and the other 8 (2%) more than 3 days later. Delay of operation was usually caused by late-diagnosis of appendicitis (Table 3), and usually resulted in longer hospital stay (p=0.000). Perforated appendicitis was significantly related to delay operation (p=0.001). Severity of appendicitis was well correlated with patient’s age (p=0.000). There was no operative death. Operative complications occurred in 11 (2.7%) patients, and 5 of them required re-operation (table 4). Discrepancies between the laparoscopic findings with pathologic reports were in 37 (9.3%) patients with suppurative or perforated appendicitis. Of 194 patients taking computed tomography, 19 (9.8%) were not compatible between the CT reports with the pathologic findings. The white cell counts and segment percents were correlated with the grading of appendicitis.

Appendicitis is an acute abdominal disease requiring urgent operation in many regional hospitals of Taiwan. A practical score system was documented in 1986, which consisting of symtoms, signs, and laboratory tests. It is useful for early diagnosis of acute appendicitis in the Department of Emergency [6]. Preoperative accurate diagnosis of appendicitis is challenging, the diagnosis must be entertained in patients presenting with an acute abdomen [7].
Based on clinical, imaging, and laparoscopic findings, a new grading system was designed [8]. But this grading system is very complicated when we try to use this system to analyze the present data. According to the data of Taiwan National Health Insurance, a total of 65,339 patients were suggestive of appendicitis during 2007 to 2009. Of them, 22,068 (33.8%) underwent LA with a lower 30-day re-admission rate [1]. In our present study, the frequency (97%) of LA was higher than other series. LA was usually associated a shorter hospital stay and lower incidence of wound infection. [2,3,9]. Mean operation time of LA could be similar or shorter comparing to the OA [3, 9]. The optimal time of appendicitis for surgery is recommended 24 to 36 hours after symptom onset, or 10 to 24 hours from admission. Delayed surgery usually prolonged the hospital length of stay [10]. There was a 2-fold increase in complication rate for patients delayed longer than 48 hours [11] or greater inpatient delay is associated with increased perforation rates [12]. Some researchers reported that 55 years was the only predictor for perforation or postoperative complications [13]. In the present study, we confirmed the delayed operation prolonged hospital stay (p=0.000), higher occurrence of perforated appendicitis (p=0.001), and the age well correlated with appendicitis severity and operative complications. Outpatient LA has been mentioned having a high rate of success, a low morbidity, and a low readmission rate [14]. Variation in outcomes by insurance status has been pointed out. The uninsured may delay seeking medical assistance, causing greater incidence of complicated disease and increased costs of treatment[15]. In Taiwan, all people have national health insurance without the above problems. We try to find out the reasons of diagnostic discrepancy of laparoscopy and pathology. The discrepancies consisted of under reading of micro-perforation or base perforation in the specimens that were treated by formalin solution, and over-reading of laparoscopic findings in cases of localized exudates. The final results were justified by repeated reading of three colleges. Abdominal CT is recommended with high sensitivity and specificity for diagnosing appendicitis [16]. In the series, 19 patients had under reading of the CT images by radiologists. In the regional hospital, laparoscopy was widely used in the treatment of appendicitis. Results of the study will provide the inter-sectional communication. Early surgery of appendicitis could reduce the operative complications.
References
- Wang CC, Tu CC, Wang PC, Lin HC, Wei PL. Outcome comparison between laparoscopic and open appendectomy: evidence from a nationwide population-based study. PLoS One. 2013;12;8
- Biondi A, Di Stefano C, Ferrara F, Bellia A, Vacante M, Piazza L. Laparoscopic versus open appendectomy: a retrospective cohort study assessing outcomes and cost-effectiveness. World Journal of Emergency Surgery 2016; 11:44
- Minutolo V, Licciardello A, Di Stefano B, Arena M, Arena G, Antonacci V. Outcomes and cost analysis of laparoscopic versus open appendectomy for treatment of acute appendicitis: 4-years experience in a district hospital. BMC Surgery 2014 14:14.
- Horvath P, Lange J, Bachmann R, Struller F, Königsrainer A, Zdichavsky M. Comparison of clinical outcome of laparoscopic versus open appendectomy for complicated appendicitis. Surg Endosc. 2017 ;31:199-205
- Masoomi H, Nguyen NT, Dolich MO, Mills S, Carmichael JC, Stamos MJ. Laparoscopic appendectomy trends and outcomes in the United States: data from the Nationwide Inpatient Sample (NIS), 2004-2011. Am Surg. 2014;80:1074-7.
- Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986;15:557-64.
- Bhangu A, Søreide K, Di Saverio S, Assarsson JH, Drake FT. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet. 2015: 26;386:1278-87.
- Gomes CA, Sartelli M, Di Saverio S, Ansaloni L, Catena F, Coccolini F, Inaba K, Demetriades D, Gomes FC, Gomes CC. Acute appendicitis: proposal of a new comprehensive grading system based on clinical, imaging and laparoscopic findings. World J Emerg Surg. 2015;10:60.
- Islam SR, Pasha K, Rahman S, Nasir E, Hanif E, Barman A. Laparoscopic vs Open Appendectomy :A Comparative Study. Bangledesh J Endosurg. 2014;2(1):5-8
- Gardiner TM, Gillespie BM. Optimal Time to Surgery for Patients Requiring Laparoscopic Appendectomy: An Integrative Review. AORN J. 2016;103:198-211
- Fair BA, Kubasiak JC, Janssen I, Myers JA, Millikan KW, Deziel DJ, Luu MB. The impact of operative timing on outcomes of appendicitis: a National Surgical Quality Improvement Project analysis. Am J Surg. 2015;209:498-502.
- Papandria D, Goldstein SD, Rhee D, Salazar JH, Arlikar J, Gorgy A, Ortega G, Zhang Y, Abdullah F. Risk of perforation increases with delay in recognition and surgery for acute appendicitis. J Surg Res. 2013 Oct;184(2):723-9
- Chen CC, Ting CT, Tsai MJ, Hsu WC, Chen PC, Lee MD, Liu MH, Shih HC. Appendectomy timing: Will delayed surgery increase the complications? J Chin Med Assoc. 2015;78(7):395-9
- Frazee RC, Abernathy SW, Davis M, Hendricks JC, Isbell TV, Regner JL, Smith RW. Outpatient laparoscopic appendectomy should be the standard of care for uncomplicated appendicitis. J Trauma Acute Care Surg. 2014;76:79-82
- Sutton TL, Pracht EE, Ciesla DJ. Acute appendicitis: variation in outcomes by insurance status. J Surg Res. 2016;201:118-25.
- Pinto Leite N, Pereira JM, Cunha R, Pinto P, Sirlin C. CT evaluation of appendicitis and its complications: imaging techniques and key diagnostic findings. AJR Am J Roentgenol. 2005;185:406-17.