


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Giant Adrenal Myelolipoma as a Rare Cause of Abdominal Pain, Case Report
Oscar Arturo Nava Carmona MD1, Medina Andrade Luis Angel MD2*, Oscar Rodrigo Rocha Erazo MD3, Rene Cano Rodriguez MD 3, Flores Galicia Hisela Viridiana MS4, Samaniego Martinez Yazmin MS4, Portillo Barranco Gonzalo Alfonso MS4, Jimenez Estevez Ivon Paulette MS4, Abundiz Holguin Isis Zahara MS4, Trejo Montaño Ivan Yanni MS4
2.General Surgery Department, General Zone Hospital #30, Iztacalco, México.
3.General Surgery Department, Military Central Hospital, México City, México.
4.Mexico Valley University, México City, México.
Copyright : © 2017 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Also known as “incidentaloma”, adrenal myelolipoma are rare adrenal tumors diagnosed once the big size of those produced symptoms of compression in other organs or an abdominal mass is evident.
Case Report: Female of 62 years-old complains for right flank pain of two months of evolution associated with urinary symptomatology and early postprandial fullness. After urinary infection treatment without improvement, an abdominal CT scan was performed and shows a heterogeneous lobulated lesion dependent of right adrenal gland, with a predominantly fat component, diameters 14 cm x 10.5 cm x 10.7 mm without significant enhancement after contrast, this lesion was displacing the right kidney and the hepatic gland. A laparotomywas performed obtaining a tumor defined by pathology as a giant adrenal myelolipoma. Patient was discharged without complications after two days.
Conclusion: Adrenal myelolipoma is a rare entity that could presents in patients with a proinflammatory state like arterial hypertension or hyperlipidemia, and for their non-functioning nature and low incidence, diagnosis could be achieved only incidentally or when their big size produces another symptomatology as in the present case.
Adrenal tumor, Myelolipoma, abdominal tumor
1. Introduction
Adrenal myelolipoma constitutes a very rare benign tumor comprising mature adipose cells and hematopoietic tissue [1] .It was initially described by Gierke in 1905 and called formations myelolipomatosis by Oberling in 1929. It is estimated that the incidence of this pathology is about 0.08 to 0.4%. In the past, the majority of this lesions were founded during autopsy, but with the widespread of non-invasive imaging studies many of them could be detected as “incidentaloma” or when their big size produce symptoms, because otherwise they course asymptomatic by their non-functional nature [2].
2. Case Report
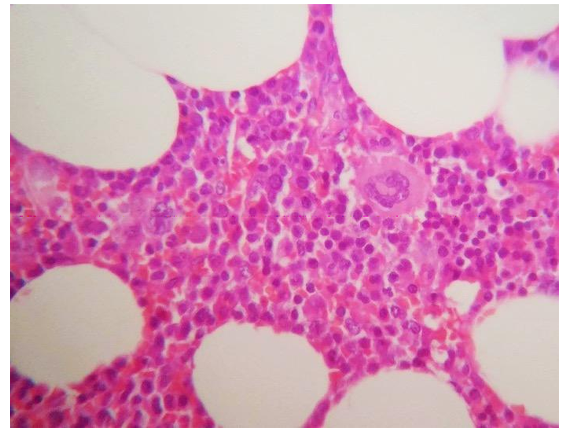
Female of 62 years-old came to emergency room complaining for a right flank pain of two months of evolution, with an intensity of 6/10 in the visual analogue scale score, associated with dysuria, oliguria, bladder tenesmus, and early postprandial fullness. Pathological background includes systemic arterial hypertension, hypertriglyceridemia and hypercholesterolemia. After urinary infection treatment in multiple occasions without improvement of symptomatology she came to the hospital. At physical exam she had Glasgow score of 15 points, blood pressure of 150/85mmHg, hearth rate of 90 beats per minute, 20 breaths per minute, with plain abdomen, normal bowel sounds, with moderate pain at palpation in right hypochondriac and flank, with a palpable mass at deep palpation, without peritoneal irritation signs. A laboratory exam presents normal values. An abdominal simple and contrasted CT scan was performed and shows a heterogeneous lesion dependent of right adrenal gland, with a predominantly fat component, diameters 14 cm x 10.5 cm x 10.7 cm in the transverse, caudal and ventrodorsal axes respectively which, after administration of contrast, shows no significant enhancement, this lesion was displacing caudally the right kidney and ventrally the hepatic gland (Figure.1). An open lumpectomy is performed without complications obtaining a tumor of 20 x 10 x 10 cm, with red-yellow color in the surface and after cut with some hemorrhagic zones (Figure.2). After pathology exam this lesion was defined as a giant adrenal myelolipoma without any other functional tissue (Figure.3). Patient was discharged without complications after two days and after three months of follow up she did not had any complications.


3. Discussion
Adrenal myelolipomais a very rare urological tumor also called “incidentaloma” by their detection in autopsy or with imaging studies in the course of non-adrenal related diseases. They have an incidence ranging between 0.08 and 0.4%, with increasing numbers by the extended use of imaging studies like ultrasound and CT scan which can detect many of them when analyzing other pathologies, but with less than 300 cases reported before 20002.
Those tumors have been related with pro inflammatory states that could precipitate adrenocortical cells metaplasia like necrosis, inflammation, infection or stress. The chronic stimulation of the gland is the main factor related with this pathology, explained by the higher incidence of lesions between sixth and seventh decade of life. Other pathologies associated with constant stimuli of adrenal gland and higher incidence of myelolipoma include Cushing`s disease, obesity, hypertension, hyperlipidemia, diabetes and stressful lifestyle [2,3].
The presentation of this tumor is asymptomatic because they are non-functional tumors, with only one case reporting a functional adenoma and their associated symptomatology; for this reason, endocrinology study is not needed frequently. The lesions are usually right sided, with predominance in males, less than 4 cm, and if they are smaller than 5 cm they should be monitored every 1-2 years with imaging controls. Contrasted CT scan appearance could show hetero mass with variable central and peripheral attenuation. Differential diagnosis should include renal angiomyolipoma, retroperitoneal lipoma, and liposarcoma. If the lesion increase in size or is bigger than 7 cm it could be removed surgically by the possibility of spontaneous rupture and hemorrhagic shock, with laparoscopic approach as the gold standard if the tumor is smaller than 7 cm. When tumor exceeds 8 cm it is called giant myelolipoma and the suggested intervention is an open lumpectomy. The tumor usually does not tend to recur after excision and for this reason have an excellent prognosis after resection [2, 4].
4. Conclusion
Adrenal myelolipoma is a very rare disease that could be presented in patients with a pro inflammatory state like arterial hypertension or hyperlipidemia. The diagnosis usually is incidental or in the context of very big tumors that generate symptomatology by compression of adjacent structures, but a correct evaluation of their non-functional nature must be confirmed prior to surgery to avoid severe complications and offer a prompt resection with the excellent associated results.
5.Acknowledgment
Thank you to Leticia Casimiro GUzman of the Pathology service for the excellent images and report.
References
- Zong-Syun Wu, MD, Shyh-Shin Chiou, MD, PhD, Wz Jui-Ying Lee, MD, and Yu-Tang Chang, MD. Intraperitoneal Accessory Spleen and Adrenal Myelolipoma: Removal by Simultaneous Bilateral Posterior Retroperitoneoscopy. Surg Laparosc Endosc Percutan Tech. February 2013; 23 (1): e29-e31
- Junaid Nabi,Danish Rafiq,Fatema N. Authoy,and Ghulam Nabi Sofi. Incidental Detection of Adrenal Myelolipoma: A Case Report and Review of Literature. Case Reports in Urology. Volume 2013, Article ID 789481, 3 pages http://dx.doi.org/10.1155/2013/789481.
- Ong K, Tan K B, Putti T. C. Myelolipoma within a non-functional adrenal cortical adenoma. Singapore Med J 2007; 48(7) : e200.
- Rashmi D Patel1, Aruna V Vanikar, Pranjal R Modi. Giant lipoma of the adrenal gland: a case report. Journal of Medical Case Reports 2011, 5:78.