


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
ARC Journal of Surgery
Volume-2 Issue-1, 2016
Abstract
Breast cancer is the most prevalent (24.1%) cancer among women. It is the second most frequent cause of cancer-deaths (18%) in women, following lung cancer. Early awareness of breast cancer by patients depends on patient’s social and educational state. Scar tissues and contractures related with burns are especially frequent in rural areas of Turkey, and they continue to be a problem. We wished to present our case, who had scar tissue development in her right breast due to burn caused by hot water at 6 years old and was diagnosed with cancer (Infiltrative ductal carcinoma, stage 3A) developing at the breast tissue under this scar 42 years old, to emphasize that patients and physicians should be mindful of cancer development under these irregular and complex tissues and to contribute in the awareness of these occurrences. Breast self-examination, mammography and physical examination are among the most emphasized topics recently. As our case developed breast cancer beneath scar tissue, we think it is a notable case to emphasize the importance of patient and public awareness.
2.INTRODUCTION
3.CASE REPORT
4.DISCUSSION
5.REFERENCES
AUTHOR DETAILS
Kazim DUMAN MD1*, Mustafa GIRGIN MD2
1*Department of General Surgery, Elazig Military Hospital, Elazig, Turkey
2Department of General Surgery, Faculty of Medicine, Firat University, Elazig, Turkey
*[email protected]
Keywords
scar tissue, early awareness, breast- self examination.
INTRODUCTION
Breast cancer is the most prevalent (24.1%) cancer among women. It is the second most frequent cause of cancer-deaths (18%) in women, following lung cancer (1). Each year, 10.000 women develop breast cancer in Turkey (2). 1/66 of all cases are in the fourth decade, and 1/40 of cases are in the fifth decade of life (3). Palpable mass in the breast is the most frequent (70%) complaint (4). Retractions, rashes and irritation in breast skin and areola are other rare signs of cancer. Early awareness of these signs by patients depends on patient‟s social and educational state. Scar tissues and contractures related with burns are especially frequent in rural areas of Turkey, and they continue to be a problem (5). We wished to present our case, who had scar tissue development in her right breast due to burn caused by hot water at young age and was diagnosed with cancer developing at the breast tissue under this scar later on her life, to emphasize that patients and physicians should be mindful of cancer development under these irregular and complex tissues and to contribute in the awareness of these occurrences.
CASE REPORT
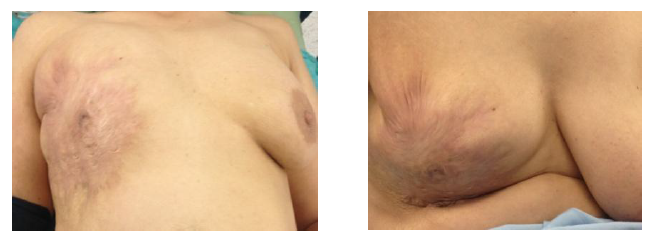
Forty-two years old female patient who had had scar tissue formation in her right breast after third degree burn with hot water when she was 5 years old, stated she felt a mass and hardness in her right breast since 3 years ago, but did not apply to a health center because she thought her complaints were related with her burn scar. She stated that the mass grew in size and she experienced increased pain within the last year, so she presented to our General Surgery Clinic. According to her medical history, there was no previous predisposing pathology related with breast cancer development. She lived in a rural area, and she was a housewife. She had attended a school for 5 years. She had had 3 normal deliveries. She did not have any relatives with breast cancer. In her physical examination, there was burn scar that covered her right breast completely (Figure- 1 and 2). There were two painful, hard and irregular surfaced mass; one was at upper-outer quadrant and was approximately 6 cm in size, and the other one was at retroareolar region and was approximately 2 cm in size. There was retraction at areola and there was fixed lymphadenopathy at right axilla.
Figure1-2. Scar that Covered Her Right Breast Completely
Mammography was technically not possible in our case. In breast ultrasonography, there were 2 lobulated, irregularly bordered, isoechogenic solid mass lesions suggesting malignancy, one at right retroareolar area and one at right upper outer quadrant, 20x20x25 mm. and 50x55x55 mm in size,respectively. At right axillary region, there were 10-12 lymphadenopathies, the largest one 15x10 mm. in size. Chest X-ray, abdominal ultrasonogram and bone scintigraphy that were performed to scan for distant metastasis did not show pathology. Tru cut biopsy from the lesion revealed malignancy. Right modified radical mastectomy was performed (Figure-3).
Figure3. Postoperative 6 Days after Right Modified Radical Mastectomy

The patient had a trouble-free postoperative period. Axillary drain was removed on third day and the patient was discharged. Histopathological examination revealed grade 3 invasive ductal carcinoma (Modified Bloom Richardson score 8, T3N3aM0), 5x5 cm in size. There was not tumor thrombosis in dermal lymphatics. There was no perineural or vascular invasion. There were metastasis in 30 of the 33 lymph nodes sampled from axilla level I and II. Eleven of the nodes were Level 2. The patient had Estrogen: 35% (+++), Progesterone (60% (+++), CerbB2: (+++), Ki67: 60% (+), E-Kadherin:(+), estrogen receptors: 90%, progesterone receptors: 60%. C-erb B-2 was negative and Ki-67 was 30% positive. In postoperative case council, adjuvant chemotherapy, radiotherapy and hormonotherapy were recommended to the patient.
DISCUSSION
Although burns caused by various causes and the resulting hypertrophic scar tissue are in the scope of plastic surgery, this topic has diverse aspects. (6). According to patient‟s own statement, she had been taken to a health center by her family at the time of burn incident. However, it had been decided that it would not pose any threat to her arm function; therefore a wound dressing had been applied, and no surgical intervention had been performed later. The patient attributed her complaints within the last 3 years to the scar tissue, so she did not apply to any health center. In Turkey, burn incidents are most commonly seen in 0-5 year age group. High incidence of burn cases in rural areas is explained by living conditions and life style, social culture, and inadequacy of health centers in these areas (5). Every individual‟s awareness should be raised against complications and aftermath of burns and the resulting scar tissue. Staging in breast cancer is performed using TNM classification which is widely accepted in the whole world. In 2002, AJCC (American Joint Committee on Cancer) accepted this classification for use in breast cancers (7). According to this classification, our case was Stage 3B, as the tumor size was 5.5cm (T3), there was involvement of internal mammarian lymph nodes (N3), and there was no distant metastasis (M0).
Stage 1 and 2 tumors are defined as early stage breast cancer, stage 3 and 4 are defined as advanced stage breast cancer. Five year survival rates go up to 100% in Stage 1 tumors, whereas 5 year survival rates are about 80% in Stage 2, 60% in Stage 3 and near 20% in Stage 4 tumors (8). This shows the importance of early diagnosis and scanning programs. In Turkey, healthy women aged between 40-69 years are scanned with mammography once in every two years. All women are recommended to perform self-breast examination after 20 years of age (9). It is planned to raise awareness of all women and population in this respect. During evaluation of patients with breast cancer, predisposing factors have great significance. Patients who have a first degree relative with breast cancer have 2.5 times greater risk. The risk is increased by 3 folds in premenopausal period, 1.3 folds if age at menarche is <12 years, 2 folds if age at menopause is >55 years, and 3 folds in nulliparous women (10). Our case developed breast cancer at premenopausal period. She did not have a history of radiation exposure or previous benign breast disease. Estrogen and progesterone receptor positivity was detected as poor prognostic indicators, while lack of vascular or lymphatic invasion and absence of protooncogene C-erb-B2 expression were good prognostic indicators for our patient.
As our case developed breast cancer beneath scar tissue, we think it is a notable case to emphasize the importance of patient and public awareness. There are many studies related to early to detection of breast cancer by patients and its significance (11). We believe studies in this field should particularly focus on rural populations. Breast self-examination, mammography and physical examination are among the most emphasized topics recently (12). Learning and application of breast self examination by women is regarded as “breast awareness” in literature; however, initial data in this regard did not yield very positive results (13). Based on non-official results, there are increasing number of authors that report these developed programs and courses have favorable outcomes regarding death rates from breast cancer (14).
REFERENCES
- Doganer YC, Aydogan U, Kilbas Z, Rohrer JE, Sari O, Usterme N, Yuksel S, Akbulut H, Balkan SM, Saglam K, Tufan T. Predictors affecting breast self-examination practice among Turkish women. Asian Pac J Cancer Prev. 2014; 15(20):9021-5.
- Ozmen V, Boylu S, Ok E, et al. Factors affecting breast cancer treatment delay in Turkey: a study from Turkish Federation of Breast Diseases Societies. Eur J Public Health. 2015 Feb; 25(1):9-14.
- Avci IA. Factors associated with breast self-examination practices and beliefs in female workers at a Muslim community. Eur J Oncol Nurs, 2008: 12: 127-33
- Robsham TE, Tretli S. Weak associations between sociodemographic factors and breast cancer: possible effects of early detection. Eur J Cancer Prev. Feb; 14(1):7-12, 2005
- Bekerecioglu M,Tercan M, Demirtas I, Atik B,Tan O. Review of Hypertrophic burn scars and its contracture. Gaziantep Med J. 2001;1:11-15
- McLean HJ. Scar Tissue. J Pastoral Care Counsel. 2015 Dec;69(4):254-7
- Singletary SE, Allred C, Ashley P, Bassett LW, Berry D, Bland KI, Borgen PI, Clark G, Edge SB, Hayes DF, Hughes LL, Hutter RV, Morrow M, Page DL, Recht A, Theriault RL, Thor A, Weaver DL, Wieand HS, Greene FL. Revision of the American Joint Committee on Cancer Staging System for Breast Cancer. J Clin Oncol 2002; 20:3628-36
- Tsukada Y, Nakamura F, Iwamoto M, Nishimoto H, Emori Y, Terahara A, Higashi T. Are hospitals in Japan with larger patient volume treating younger and earlier-stage cancer patients? An analysis of hospital-based cancer registry data in Japan. Jpn J Clin Oncol. 2015 Aug;45(8):719-26
- OZMEN V Breast Cancer in Turkey Turkiye Klinikleri J Gen Surg-Special Topics 2013;6(2):1-6
- Ambrosone CB, Hong CC, Goodwin PJ. Host Factors and Risk of Breast Cancer Recurrence: Genetic, Epigenetic and Biologic Factors and Breast Cancer Outcomes. Adv Exp Med Biol. 2015;862:143-53
- Abolfotouh MA, BaniMustafa AA, Mahfouz AA, Al-Assiri MH, Al-Juhani AF, Alaskar AS. Using the health belief model to predict breast self examination among Saudi women. BMC Public Health. 2015 Nov 23; 15(1):1163.
- Thomas DB, Gao DL, Ray RM, Wang WW, Allison CJ, Chen FL, et al. Randomized trial of breast self-examination in Shanghai: final results. J Natl Cancer Inst. 2002; 94(19):1445–57.
- Kosters J, Gotzsche P. Regular self-examination or clinical examination for early detection of breast cancer. Int J Epidemiol. 2008; 37(6):1219.
- Thornton H, Pillarisetti RR. „Breast awareness‟ and „breast self-examination‟ are not the same. What do these terms mean? Why are they confused? What can we do? Eur J Cancer. 2008; 44(15):2118–21.