


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Influence of Age-Related Karate Training on Gait Variability under Dual-Task Conditions- A Controlled Study
Gerald Pliske1,2*,Peter Emmermacher1,Nicole Bandow1,Stefan Piatek2,Veronika Weinbeer1,Kerstin Witte1
2.Department of Traumatology, Otto-von-Guericke University, Magdeburg, Germany.
Copyright :© 2017 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Purpose: Increased gait variability is an indicator of a increased tendency to fall and can be seen as a predictor of future falls among older people. Aim of the present study was to explore the influence of karate training on the gait variability under normal walking and dual-task conditions.
Methods: In this randomized, controlled study 44 participants, aged between 62 and 74, participated in a karate training twice a week for 5 months. A gait analysis including a cognitive (CDT) and a motor dual-task (MDT) condition was performed before and after the intervention. The following gait parameters were evaluated: cadence, walking speed, step time and step length.
Results: The intervention showed a significant reduction in variability for cadence, walking speed and step time under cognitive dual-task condition. Furthermore, a decrease in variability for step time and step length under MDT condition could be observed.
Conclusions: Karate seems to be useful to reduce gait variability among older people under dual-task conditions and could be utilized as a fall prevention program.
Elderly, fall prevention, gait analysis, karate, variability, dual-task,Research in Sports Medicine
1. Introduction
Falls among elderly people during locomotion are a prominent health issue and accompanied by high economic costs [1]. The causes of falls are manifold and reach from physiological factors like cognitive, sensory and muscle function to extrinsic factors such as uneven underground or poor lighting conditions [2]. The cause of a fall can also lie within an uncertain gait, which is often observed in elderly people. Besides the spatiotemporal gait parameters, it could be helpful to assess the gait pattern’s variability and detect an increased risk for falls. The linear variability of temporal measures of swing and stance, for instance, is an appropriate parameter to distinguish between fallers and non-fallers [3-6]. Increased variability can be observed at people who had a stroke but it can also be noted at healthy people [5]. Reduced mediolateral stability under dynamic conditions like walking can be seen from fourth or fifth decade [7].
The upright gait is mainly controlled by the spinal cord and sub cortical regions of the cerebrum [8]. This system and so the gait variability as well, can be influenced by various internal and external factors like diseases of the central nervous system or competing cognitive or motor tasks [9]. It can be assumed that the gait variability increases if the single task “gait” is perturbed by a second task [10]. People, who are distracted by a second task, such as a cognitive or a motor task, cannot concentrate on their gait. Furthermore, it could be shown that older people have a larger center-of-pressure displacement and a greater stride-to-stride variability under dual-task conditions [11]. While among healthy young adults a special concentration on the gait pattern is not necessary, the focus must be increasingly directed towards the gait at increasing age.
Gait parameters and variability can be trained under single- and dual-task conditions. In a systematic review 22 studies showed that dual- task training can improve the dual-task postural control to some extent. While single task training showed a positive influence on balance or walking none was reported on dual-task postural control [12]. It seems that an intervention with combination of motor and cognitive elements can be useful to improve gait performance, reduce gait variability and hence decrease the risk of falling. Sports inheriting such cognitive and physical aspects are martial arts. Martial arts have frequently been used to improve gait or dual-task performance. For example, Manor et al. (2014) showed that the walking speed under single and dual-task conditions increases after 12 weeks of Tai Chi training compared to a control group [13]. Wayne et al. (2015) compared Tai Chi experts with Tai Chi beginners and showed that the stride time variability was lower in the expert group [14]. Karate, as a specific type of martial arts, contains holistic movements that improve strength, endurance and balance. Single movements (punches and kicks) are already well defined and need exact execution. The positive effect of other sports (e. g. dancing) on gait variability and dual-task performance has been proved in other studies [15]. Further interventions with cognitive and motor exercises reduced the step time variability, the gait variability in DT-situations and the fall frequency of over 70 year old people with cognitive impairment [15]. A reduced fall rate for community dwelling survivors of stroke with a mean age of 70 years could be observed after a 12-week Tai Chi intervention [16]. In a meta-analysis positive effects of Tai Chi on balance and the fear of falling are reported, additionally [17].
In regard to the analysed participants and used field of sports, most of the studies focused on impaired people and used the special type of martial arts: Tai Chi. Up to now, no study has analyzed the influence of karate training on the human gait of healthy community dwelling people over 65 years. Aim of this study therefore was to determine the effect of a 5 months karate training on gait variability among elderly people. The execution of karate specific movements could be able to increase the variabilities for spatiotemporal gait parameters like cadence, walking speed, step time and step length. It can be shown that cognitive requirements such as simultaneously counting and karate related movements or responding to an opponent has an influence on DT performance and also reduces the second task’s effect on gait performance.
2. Methods
The study was conducted in accordance to the guidelines proposed by the Declaration of Helsinki. The participants were acquired through the local newspaper. A positive vote by the Ethics Committee (Otto-von-Guericke University Magdeburg, Germany, registration number: 109/11) was given. The study was supported by the Otto-von-Guericke University Magdeburg, Germany. 44 participants aged between 62-74 years (mean age 69.14 years ± 4.10) were included in the study. All participants were community dwelling healthy people. Participants with severe chronic diseases such as not adjustable diabetes mellitus, coronary heart disease with signs of instability, myocardial infarction or stroke, artificial joints but also participants which had gained experience in karate sports or other martial arts in the past twenty years were excluded. Before the study started, the participants had to fill out a questionnaire regarding their own physical activity and personal fall history over the past 12 months. The participants were randomized by draw and split into the karate group [n = 25] (KG) and the control group [n = 19] (CG). The participants had to at least attend 80% of the intervention, otherwise they were excluded (Table 1).
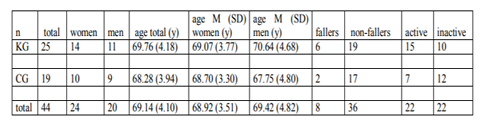
Descriptive statistics of the participants including gender, age, and history of falls in the last 6 month before the study and activities organized in sport clubs No significant differences between the groups concerning age (KG: Mean (M) = 69.76, standard deviation (SD) = 4.1; CG: M = 68.28, SD = 3.9; t-test: F = 0.004, df = 41, p = 0.247), gender composition (KG: ♂ = 11 ♀ = 14; CG: ♂ = 9, ♀ = 10; two-dimensional chi-squared test: χ2 (Pearson) = 0.049, df = 1, p = 0.824; χ2 (Likelihood quotient = 0.049, df = 1, p = 0.824)), falls in the past (two-dimensional chi-squared test: χ2 (Pearson) = 0.460, df = 1, p = 0.498) and physical activity level (two-dimensional chi-squared test: χ2 (Pearson) =
1.014., df = 2, p = 0.602) were found.
The workouts were performed in the gymnasium of the Otto-von-Guericke University Magdeburg, Germany over 5 months with 2 units per week, 60 minutes each. The karate training was guided by experienced karate instructors and contained age-related movement executions [18]. Elements of each single karate training were warm up, basic techniques with punches, kicks, stances, defense techniques as well as kata performance (choreographed patterns of techniques against an imaginary enemy) and cool down. Real kumite (fight practice) and fall school were no elements of training, due to the high risk of injuries. Dual-task conditions were implemented through the combination of counting repetitions and basic karate techniques and or by simultaneously performing a kata. The CG was instructed to not change their sport behavior during the intervention time.
Kinematic gait parameters were recorded by motion capturing (VICON system with 12 MX cameras, company Vicon Ltd., Oxford, UK) in a gait laboratory [size 6m * 4m * 3.5m] using the full body Plug-In-Gait marker set.
The participants had to walk along a circular course [9.0 m * 5.0 m] ten times for each condition (normal walking, cognitive dual-task and motor dual-task). Only the trials on the long straights of the circle course were integrated in the evaluation. At least 20 double steps of the left leg per task and person were recorded. A double step was defined from foot off to heel strike of the left foot.
First, the participants had to walk the course at a self-selected speed with their ordinary walking style (NW). Second, they had to walk and consistently subtract the value “3” from a given number (pre-test 271 and post-test 272) was the cognitive dual-task condition (CDT). Each result had to be spoken out loud [19]. The number of correct and incorrect results was recorded.
The third task was to simultaneously walk and carry a cup of water, called motor dual-task (MDT) [20,21]. The walking speed during the CDT and MDT was self-selected.
The examined temporal gait parameters were cadence, walking speed, step time and the spatial gait parameter was step length for the normal walk, CDT and MDT. The gait variability is a combination of both characteristics and can be described as spatiotemporal gait parameter and was calculated by using the formula: CV = SD /MW * 100.
The statistical analysis was performed using IBM SPSS Statistics 20 and Microsoft Excel 2006.
Normal distribution was verified by using the Kolmogorov-Smirnov test. The paired t-test was used to compare the parameters of the pretest and posttest. For samples which were not normally distributed were analyzed with the Wilcox on test. The one-way ANOVA or the Friedman tests were, with 5% significance level, used to compare all walking conditions among each other (NW, CDT, and MDT).
The primary endpoints of the study were the reduction of the gait variability for the KG for normal walk, CDT and MDT in general and specific the reduction of the influence of the second task (cognitive or motor) on the gait variability parameters measured during gait analysis.
3. Results
Only participants of the KG with at least 60% of attendance were taken into account for evaluation. In average the attendance was more than 80%. The results of the gait analysis including the mean values and standard deviations of the gait parameters cadence, walking speed, step time and step length are published by Pliske et al. 2015 [22].
All gait parameters were checked for significant differences between both groups before the intervention. The baseline conditions for both groups and under all walking task conditions concerning the tested gait parameters and the characteristics of the participants did not differ from each other. All participants started the intervention on an equal footing.
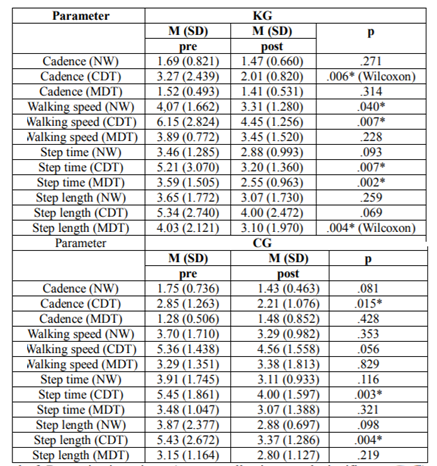
Data are expressed as mean ± standard deviation (M ± SD). Table 2 shows that the KG was able to lower the variability under CDT conditions significantly for cadence (M = 3.27 ± 2.44 and M = 2.01 ± 0.82, p = 0.006), walking speed (M = 6.15 ± 2.82 and M = 4.45 ± 1.26, p = 0.007) and step time (M = 5.21 ± 3.07 and M = 3.20 ± 1.36, p = 0.007). A significant change in variability for CG under CDT conditions could be seen for cadence (M = 2.85 ± 1.26 and M = 2.21 ± 1.08, p = 0.015), step time (M = 5.45 ± 1.86 and M = 4.00 ± 1.60, p = 0.003) and step length (M = 5.43 ± 2.67 and M = 3.37 ± 1.29, p = 0.004). Furthermore, a significant reduction of the gait variability could be achieved by the KG concerning step time (M = 3.59 ± 1.50 and M = 2.55 ± 0.96, p = 0.002) and step length (M = 4.03 ± 2.12 and M = 3.10 ± 1.97, p = 0.004) under MDT condition. Under NW conditions the KG was able to reduce the variability for walking speed (M = 4.07 ± 1.66 and M = 3.31 ± 1.28, p = 0.040).
Significant results were found for NW and CDT for the karate group (KG). When comparing NW and CDT in the pre-test a significant difference could be observed for the variability of cadence parameters (M = 1.68 ± 0.82 and M = 3.27 ± 2.44, p = 0.002) (Table 3). This significant difference between NW and CDT for the variability of cadence could not been observed anymore in the post-test.
Results of the one-way ANOVA and Friedman test (F) between NW, CDT & MDT. After Bonferroni correction the following results are significant (*) (p< 0.05).
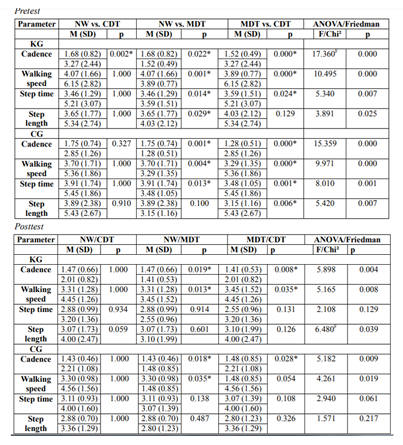
The comparison between NW and MDT in the KG shows significant differences in variability of cadence (M = 1.68 ± 0.82 and M = 1.52 ± 0.49, p = 0.022), for walking speed (M = 4.07 ±
1.66 and M = 3.89 ± 0.77, p = 0.001), for step time (M = 3.46 ± 1.29 and M = 3.59 ± 1.51, p = 0.014) and for step length (M = 3.65 ± 1.77 and M = 4.03 ± 2.12, p = 0.029). After the
intervention only the variability of cadence (M = 1.47 ± 0.53 and M = 1.41 ± 0.53, p = 0.019) and walking speed (M = 3.31 ± 1.28, p = 0.013 and M = 3.45 ± 1.52, p = 0.013) still differ significantly.
The initial significant differences of variability of step time (M = 3.59 ± 1.51 and M = 5.21 ± 3.07, p = 0.024) in the pretest could not been observed in the posttest anymore. The significant differences for cadence (M = 1.52 ± 0.49 and M = 3.27 ± 2.44, p = 0.000) and walking speed (M = 3.89 ± 0.77 and M = 6.15 ± 2.82, p = 0.000) were still present in the posttest (cadence M = 1.41 ± 0.53 and M = 2.01 ± 0.82, p = 0.008) (walking speed M = 3.45 ± 1.52 and M = 4.45 ± 1.26, p = 0.035).
No significant differences between NW and CDT could be found for the variability of the measured gait parameters between pre- and post test.
The initial significant difference of the step time variability (M = 3.91 ± 1.74 and M = 3.48 ± 1.05, p = 0.013) could not be observed in the posttest anymore. The significant differences for the variability of cadence and walking speed remained stable.
In the pre test all measured gait parameters showed significant differences between MDT and MDT. In the post test only the variability of cadence still differs significant from each other (M = 1.48 ± 0.85 and M = 2.21 ± 1.08, p = 0.028). For the variability of walking speed, step time and step length no significant differences could be observed in the posttest.
The influence of a DT situation on cadence seems to be stable and may need a longer period of training for a significant change. The significant differences for cadence between NW/MDT and MDT/CDT could not be erased through the intervention.
After the intervention there was only a significant difference for step time under MDT condition between the groups (p = 0.042, df = 2, F = 3.209). The remaining parameters and the other two walking conditions showed no significant differences.
4. Discussion
Gait instability and associated gait variability can be part of an increased risk of falling in old age [23]. On several occasions it has been attempted to reduce the gait variability through sport interventions, for example martial arts like Tai Chi [24]. Up to now, the effect of karate on gait variability under single and dual-task conditions is unknown. In this randomized and controlled study, the effect of a 5 months karate training for healthy people over 65 years on the gait variability should be examined. It could be shown that the training reduced especially the gait variability for the temporal gait parameters walking speed under single task walking conditions, cadence, walking speed and step time under CDT and step time under MDT conditions. Furthermore, the variability of the spatial gait parameter step length was effected by the karate intervention.
Comparing the pre- and post-test, the KG could reduce the variability of cadence, walking and step time under CDT conditions significantly. Likewise, the step time and step length improved under MDT conditions. Similar results were found in the study of Gregory et al., where healthy people accomplished a combined exercise and dual-task training for 26 weeks and showed an increased gait velocity and reduced stride time variability under DT-conditions [25].
In the present study no changes are found for the normal gait after the intervention. In summary, it can be stated that most significant changes are within temporal gait parameters under CDT conditions. For the KG the temporal gait parameters cadence, walking speed and step time showed significant improvements after the intervention. But also the CG showed significant changes in the variability of cadence and step time under CDT. Under normal walking conditions the KG improved the walking speed and also the step time variability under MDT conditions. At this point it has to be mentioned that only one spatial parameter was measured. That increases the probability that changes appear in temporal parameters. The results of the present study show that only step length of the KG under MDT conditions improved significantly. The measurement of only one spatial gait parameter is a clear limitation of the study. In future studies, further spatial gait parameters like the foot angle or the stride width could be measured in order to make a better statement about the influence of an intervention on spatial gait parameters [26].
Our findings show that gait variability under CDT conditions seems to decrease after 5 months of karate intervention. These results are in contrast to the study by Beauchet et al. (2013), where 48 community dwelling people (mean age 72.2 ± 8 years) participated a three month physical training program to improve gait variability under single and dual-task conditions. After the intervention the stride time could be significantly reduced under single task but not under dual-task condition [27]. On the other hand the study of Beauchet et al. is in contrast the study from Wang et al. in which 29 community dwellers absolved a combined exercise with resistance, endurance and balance training for 12 weeks. The intervention group showed a significant reduction of the stride time and stride length variability [28].
Furthermore, a DT-situation has also strong influence on the gait variability and leads to an increased risk of falling. It could be shown that external confounders like mechanical or visual influences lead to an increased step width and step length variability [29], while external stabilization leads to a decrease in step with variability [30].
In regard to CDT a significant influence for the intervention group can be found in this study. That might suggest that a cognitive component of training could be helpful to reduce the gait variability and increase the CDT performance [31,32]. This effect occurred in particular for the temporal gait parameters cadence, walking speed and step time.
Step width variability was used to differ between people with higher and lower risk of falling [33]. In other studies, no difference between fallers and non-fallers occurred for step width variability [34]. In a follow-up study the influence of a karate intervention on the step width should be tested.
The improvements of step time and step length variability in this study indicate that the participants made larger strides with a secure gait after the intervention. Similar observations could not be made in the CG.
However, the CG could improve their cadence, step time and step length under CDT without any kind of intervention from pretest to posttest. Besides, the CG could also eliminate the initial differences between NW/MDT for step time and additionally for step length between MDT/CDT.
The same occurred for the KG. There were no significant differences between NW/MDT for step time and step length and between MDT/CDT for step time. Furthermore, the KG could erase the initial difference of the cadence between NW/CDT after 5 months of training.
The findings of the CG could result from the reduced test-retest reliability in elderly people [35]. The enhancements of the CG could also be a consequence of a habituation to the tests and measurements made. To avoid this problem a gait analysis could be performed before the study so the participants could get used to the test situation. A lack of the familiarization procedure is another limitation of the present study.
In accordance with other studies, it is also possible that longer intervention times and more gait analysis during the intervention is needed to see a clear difference between the intervention-and the control group [27,36]. It might also be that the participants of the CG did not follow the study instructions and changed their activities in their leisure time. Furthermore, it must be stated that most intervention studies with martial arts are performed with impaired people or residents of nursing homes.
It seems that more than 100 steps per participant and condition for evaluating the gait variability should be captured in future studies. Ten to twenty steps may reliable measure for the mean values of velocity and cadence [37].
Martial arts and more specifically karate seem to be suitable to reduce the risk of falling during dual-task situations due to a reduction of the variability of the temporal gait parameters. It seems that it needs a longer time of intervention to see the positive effects of karate on gait variability of healthy elderly people. Consequently, the training should be carried out with impaired people to highlight the impact of karate on the gait of elderly in future studies. May be karate can show his potential as a tool for secondary fall prevention and not as primary prevention for healthy community dwellers.
References
- Heinrich S., Rapp K., Rissmann U., Becker C. and Künig H. H., Costs of falls in old age: a systematic review, Osteoporos Int. 21, 891-902 (2010). doi:10.1007/s00198-009-1100-1
- Ambrose A. F., Cruz L. and Paul G., Falls and Fractures: A systematic approach to screening and prevention, Maturitas. 82, 85-93 (2015).
- Hamacher D., Singh N. B., Van Dieën J. H., Heller M. O. and Taylor W. R., Kinematic measures for assessing gait stability in elderly individuals: a systemic review, J. R. Soc. Interface. 8, 1682-1698 (2011).
- Mansfield A., Wong J. S., McIlroy W. E., Biasin L., Brunton K., Bayley M. and Inness E. L., Do measures of reactive balance control predict falls in people with stroke returning to the community?, J. Physio. 8 (2015). doi: 10.1016/j.physio.2015.01.009
- Brach J. S., Perera S., Studenski S., Katz M., Hall C. and Verghese J., Meaningful change in measures of gait variability in older adults, Gait Posture. 31, 175-179 (2010).
- Callisaya M. L., Blizzard L., Schmidt M. D., Martin K. L., McGinley J. L., Sanders L. M. and Srikanth V. K., Gait, gait variability and the risk of multiple incident falls in older people: a population-based study, Age Ageing. 40, 481-487 (2011).
- Terrier P. and Reynard F., Effect of age on the variability and stability of gait: A cross-sectional treadmill study in healthy individuals between 20 and 69 years of age, Gait Posture. 41, 170-174 (2015).
- Shik M. L. and Orlovsky G. N., Neurophysiology of Locomotor Automatism, American Physiological Society. 56 (3), (1976).
- Granacher U., Mühlbauer T., Bridenbaugh S., Wehrle A. and Kressig R. W., Age-Related Differences During Single and Multi-Task Walking, German J. Sports Med. 61 (11), 258-263 (2010).
- Steinmetz J. P. and Federspiel C., The effects of cognitive training on gait speed and stride variability in old adults: findings from a pilot study, Aging Clin. Exp. Res. 26, 635-643 (2014).
- Granacher U., Bridenbaugh S. A., Muehlbauer T., Wehrle A. and Kressig R. W., Age-Related Effects on Postural Control under Multi-Task Conditions, Gerontology 57, 247-255 (2011).
- Agmon M., Belza B., Nguyen H. Q., Logsdon R. G. and Kelly V. E., A systematic review of interventions conducted in clinical or community settings to improve dual-task postural control in older adults, Clin. Interv. Aging. 9, 477-492 (2014).
- Manor B., Lough M., Gagnon M. M., Cupples A., Wayne P. M. and Lipsitz L. A., Functional benefits of Tai Chi training within senior housing facilities, J. Am. Geritar. Soc. 62 (8), 1484-1489 (2014).
- Wayne P. M., Hausdorff J. M., Lough M., Gow B. J., Lipsitz L., Novak V., Macklin E. A., Peng C. K. and Manor B., Tai Chi training may reduce dual task gait variability, a potentional mediator of fall risk, in healthy older adults: cross-sectional and randomized trial studies, Front. Hum. Neurosci. 9 (2015). doi:10.3389/fnhum.2015.00332
- Eggenberger P., Theill N., Holenstein S., Schumacher V. and de Bruin E. D., Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: a secondary analysis of a 6-month randomized controlled trial with 1-year follow-up, Clin. Interv. Aging 10, 1711-1732 (2015).
- Taylor-Piliae R. E., Hoke T. M., Hepworth J. T., Latt L. D., Najafi B. and Coull B. M., Effect of Tai Chi on physical function, fall rates and quality of life among older stroke survivors, Arch. Phys. Med. Rehabil. 95 (5), 816-824 (2014).
- Park M. and Song R., Effects of Tai Chi on fall risk factors: a meta-analysis, J. Korean Acad. Nurs. 43 (3), 341-351 (2013).
- Emmermacher P. and Witte K., Exercise in a different way—fall prevention as well as maintaining and improving of learning and memory performance in older adults by East Asian martial arts, 1st ed. Aachen,Germany: Shaker, 2012, ch. 1-3.
- Priest A. W., Salamon K. B. and Hollman J., Age-related differences in dual task walking: a cross sectional study, J. Neuroeng. Rehab. (2008). doi:10.1186/1743-0003-5-29
- Bridenbaugh S. A. and Kressig R. W., Motor cognitive dual tasking: early detection of gait impairment, fall risk and cognitive decline, Z. Gerontol. Geriatr. 48 (1), 15-21 (2015).
- Laessoe U., Hoeck H. C., Simonsen O. and Voigt M., Residual attentional capacity amongst young and elderly during dual and triple task walking, Hum. Move. Sci. 27 (3), 496–512 (2008).
- Pliske G., Emmermacher P., Weinbeer V. and, Witte K. Changes in dual-task performance after 5 months of karate and fitness training for older adults to enhance fall prevention, Aging Clin. Exp. Res. 28 (6), 1179-1186 (2015).
- Roos P. E. and Dingwell J. B. Using dynamic walking models to identify factors that contribute to increased risk of falling in older adults, Hum. Mov. Sci. 32, 984-996 (2013).
- Graveson J., Bauermeister S., McKeown D. and Bunce D., Intraindividual Reaction Time Variability, Falls and Gait in Old Age: A Systematic Review, J. Gerontol. (2015). doi:10.1093/geronb/gbv027
- Gregory M. A., Gill D. P., Zou G., Liu-Amborse T., Shigematsu R., Fitzgerald C., Hachinski V., Shoemaker K, and Petrella R. J., Group-based exercise combined with dual-task training improves gait but not vascular health in active older adults without dementia, Arch. Gerontol. Geriatr. 63, 18-27 (2015).
- Rigas C. Spatial parameters of gait related to the position of the foot on the ground, Prosthetics and Orthotics International 8, 130- 134 (1984).
- Beauchet O., Launay C., Annweiler C., Fantino B., Allali G. and De Decker L., Physical training-related changes in gait variability while single and dual tasking in older adults: magnitude of gait variability at baseline matters, Eur. J. Phys. Rehabil. Med. 49 (6), 857-864 (2013).
- Wang R. Y., Wang Y. L., Cheng F. Y., Chao Y. H., Chen C. L. and Yang Y. R., Effects of combined exercise on gait variability in community-dwelling older adults, Age 37 (3), (2015). doi: 10.1007/s11357-015-9780-2
- McAndrew P. M., Dingwell J. B. and Wilken J. M., Walking variability during continuous pseudo-random oscillations of the support surface and visual field, J. Biomech. 43, 1470-1475 (2010).
- Donelan J. M., Shipman D. W., Kram R. and Kuo A. D., Mechanical and metabolic requirements for active lateral stabilization in human walking, J. Biomech. 37, 827-835 (2004).
- An H. J., Kim J. I., Kim Y. R., Lee K. B., Kim D. J., Yoo K. T. and Choi J. H., The Effect of Various Dual Task Training Methods with Gait on the Balance and Gait of Patients with Chronic Stroke, J. Phys. Ther. Sci. 26, 1287-1291 (2014).
- Shin S. S. and An D. H., The Effect of Motor Dual-task Balance Training on Balance and Gait of Elderly Women, J. Phys. Ther. Sci. 26, 359-361 (2014).
- Brach J. S., Berlin J. E., Vanswearingen J. M., Newman A. B. and Studenski S. A., Too much or too little Step width variability is associated with a fall history in older persons who at or near to normal gait speed, J. Neuroeng. Rehabil. 2 (21) (2005). doi:10.1186/1743-0003-2-21
- Moe-Nilssen R. and Helbostad J. L., Interstride trunk acceleration variability but not step width variability can differentiate between fit and frail older adults, Gait Posture 21, 164-170 (2015).
- Almarwani M., Perera S., VanSwaeringen J. M., Sparto P. J. and Brach J. S., The test-retest reliability and minimal detectable change of spatial and temporal gait variability during usual over-ground walking for younger and older adults, Gait Posture 44, 94-99 (2016).
- Choi J. S., Kang D. W., Seo J. W. and Tack G. R., Reliability of the walking speed and gait dynamics variables while walking on a feedback-controlled treadmill, J. Biomech. 48, 1336-1339 (2015).
- Hollman J. H., Childs K. B., McNeil M. L., Mueller A. C., Quitter C. M. and Youdas J. W., Number of strides required for reliable measurements of pace, rhythm and variability parameters of gait during normal and dual task walking in older individuals, Gait Posture 32 (1), 23-28 (2010).