


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Measurement of Head Impacts in a Senior Amateur Rugby League Team with an Instrumented Patch: Exploratory Analysis
Doug King1,2*,Hume1,3,Gissane4,Cummins2,Clark5
2.School of Science and Technology, University of New England, Armidale, NSW, Australia.
3.National Institute of Stroke and Applied Neuroscience (NISAN), Faculty of Health and Environmental Science, Auckland University of Technology, Auckland, New Zealand .
4.School of Sport Health and Applied Science, St Mary’s University, Twickenham, Middlesex, United Kingdom.
5.Australian College of Physical, Education Faculty of Sport Performance Sydney Olympic Park NSW, Australia.
Copyright :© 2017 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Accelerometer devices can quantify the magnitude of head impacts during sport to ascertain potential for brain injury. There are no published head impact data for rugby league. The objective of this study was to quantify head impacts for amateur senior rugby league players to ascertain potential for brain injury. Data on head impact magnitude, frequency and distribution were collected with instrumented behind-the-ear XPatches (accelerometers) worn by 42premier senior amateur rugby league players participating in 2014 and 2015 domestic seasons of matches. During the study there were20, 837 impacts >10g recorded. The mean number of impacts per player over the season was 672±237resulting in 52 ±79 impacts to the head per player, per match. Players recorded a median [IQR] linear (14 [10 to 23] g), and rotational (3,181 [1830 to 5,612] rad/s2) accelerations over the study. Over the study there were 103 impacts (0.5%) for linear acceleration, and 4,505 impacts (22%) for rotational acceleration, above previously published linear and rotational injury tolerance thresholds. The median peak linear acceleration of 14gwaslower, while the median rotational acceleration of 3,181 rad/s2was higher than the medians reported in American high school football, collegiate football and youth ice hockey. The potential for brain injury in rugby league players as indicated by head impact acceleration is likely similar to American football and rugby union. Given world-wide growth of rugby codes, sports clinicians need to be aware of the potential for head injury and likely concussion prevention and management options.
Key points:
• Linear acceleration characteristics for head impacts per player per game for rugby league were similar to those reported for American high school football, collegiate football and youth ice hockey.
• Rotational acceleration characteristics for head impacts per player per game for rugby league were higher than those reported for American high school football, collegiate football and youth ice hockey.
• The majority of linear and rotational acceleration impacts recorded in senior amateur rugby league fell into the mild category of impact severity.
Injury, Linear Acceleration, Rotational Acceleration, Head Impact, Rugby League,Research in Sports Medicine
1. Introduction
Played at junior, amateur, semi-professional and professional levels,[1] rugby league is an intermittent collision sport involving numerous collisions and tackles. 1 Played with 13 players on-field, with 4 reserves, the game is typically (but not always) played under a limited interchange rule where up to 12 interchanges of players are permitted in matches. Each team is permitted six tackles in possession of the ball with which they must advance into the opposition’s territory and score a try. 2-4 The ball must only be passed backwards but can be carried or kicked into the opposition’s territory. 2, 4 At the completion of six tackles the ball is immediately given to the opposition team to commence their set of six tackles.[2,3] Most teams often kick the ball after the fifth tackle (ceding the possession to the opposition) to avoid being tackled a sixth time, in an attempt to gain further territorial advantage. The same players are therefore involved in both attack and defence.
At the professional level of rugby league, players can experience from 34 to 72 tackle situations per match either as the tackler or the ball carrier.[5] As a result of the tackle situations, many impacts to the body and head occur from match participation in rugby league. Knowledge of the potential metabolic and ultra structural consequences of impacts to the head has grown, as has the appreciation for repetitive concussive and subconcussive impacts and the possible deleterious effects in some individuals [6].Technology, such as accelerometers in the helmets of American football players, [7-9]and New Zealand amateur rugby union players[10] have increased the knowledge and analysis of injury biomechanics of the forces, accelerations, frequencies and velocities of head injuries[11].
Despite more studies reporting impacts to the head and concussions, none have identified a data acquisition threshold that constitutes where a subconcussive impact occurs. Impacts under 10g are reported[12]to be a result of non-contact activities such as walking, jumping, running and sitting.[13] Impacts over 10gthat do not result in a participant presenting with acute signs or symptoms of concussion, have been identified to be subconcussive impacts[14]. Repetitive subconcussive impacts may have negative long-term effects.[15] Several studies have utilized data acquisition thresholds greater than 10g(i.e. 14.4g,[16-18] 15g7, [19,20] and 30g6) to report findings and may have removed a large number of subconcussive impacts from their dataset. The data obtained from these types of impacts is not normally distributed. Non-helmeted sports have utilized accelerometers in measuring impacts from sports participation. Heading the ball by female soccer youths yielded peak accelerations of 63g and 8,869 rad/s2.21 No concussions were reported,[21] as no injury nor injury risk was assessed; even though some of the rotational accelerations were within the nominal values for an injury to the head when compared with American football data[22] and injury risk tolerance levels. [23]Although head impact data are accumulating for soccer,[24,25]ice hockey, [26-28]American football[29]rugby union[30]and junior[31] and women’s[32] rugby league, there are no published head impact data for male senior amateur rugby league. Given that rugby league is a different contact sport when compared to rugby union, there is a need to explore the impacts to the head within this sporting code. Therefore, this study quantified impacts to the head via an instrumented patch worn behind the ear for amateur rugby league players over two premier seasons of domestic matches in New Zealand.
2. Methods
A cross-sectional study was conducted on a senior club level amateur rugby league team over two competitive seasons (2014, 2015) in New Zealand. There were 33 players enrolled in 2014 and 35 players enrolled in 2015. The majority of the players (78.7%) played in both competition seasons. A total of forty-two players were enrolled in the study with a mean ±SD age, body mass and height of 23.3 ±4.3 yr. 93.6 ±14.4 kg and 1.80 ±0.05 m. The players were considered amateur receiving no remuneration for participating in rugby league activities. The matches were played under the laws of New Zealand Rugby League. Players were placed into three positional groups: (1) hit-up forwards (n= 4: 2 x prop, 2 x second row); (2) outside backs (n= 5: 2 x centre, 2 x wing and fullback); and (3) adjustables (n= 4: hooker, halfback, five-eight, and loose forward).33The researcher’s university ethics committee (AUTEC 12/156) approved all procedures in the study and all players gave informed consent prior to participating in the study.
Every player wore the XPatch impact-sensing skin patch (X2Biosystems Ltd, Seattle, Washington. United States of America; www.x2biosystems.com) on the skin covering their right-side mastoid process during each match sampling at 1,024 Hz. The positioning of the XPatch over the mastoid process is important to ensure that the sensor was not activated by enhanced soft-tissue effects when impacts occur25 and was placed on the players by the lead researcher 15 minutes prior to the match starting. The XPatch contained a low-power, high-g triaxial accelerometer with 200g maximum per axis and a triaxial angular rate gyroscope to capture six degrees of freedom for linear acceleration and rotational velocity. The XPatch calculated rotational acceleration of the heads’ centre of gravity for all impacts that occurred during matches. The time history incorporated three axes (x, y, z) of acceleration and three axes of velocity. Standing in an upright position these planes describe the medial-lateral, anterior-posterior and vertical acceleration and deceleration.
A data acquisition limit of 10g10, 34 was utilised for the study. If an impact exceeded the predetermined 10g linear acceleration threshold, 100 milliseconds (ms) of data (10 ms pre-trigger and 90 ms post-trigger) from each accelerometer and gyroscope were recorded to the on-board memory for later downloading. All matches were videotaped (Sony HDR-PJ540 Camcorder) to enable verification of the impacts recorded. The time stamp of the match was synchronized with the X2 XPatch prior to very game.
Following the match, the XPatch was removed from each player and downloaded to the Injury Management Software (IMS) (X2Biosystems). The IMS enabled the raw accelerometer data to be transformed to the head centre of gravity by using a rigid-body transformation for linear acceleration and a 5-point stencil for rotational acceleration.10, 25 The biomechanical measures of head impact severity consisted of peak linear acceleration (g), and peak rotational head acceleration (rad/s2).35 False impacts were removed by the X2Biosystems proprietary ‘de-clacking’ algorithm10 by comparing the waveform of each impact to a ‘Gaussian-like’ reference waveform using cross-correlation. 10The XPatch impact data were adjusted to enable correlation with a head form criterion standard as previously reported. 36Impacts with a peak linear acceleration of < 10gwere removed. The remaining impacts to the head were downloaded to an Excel 2016 spreadsheet and time-filtered to include only those impacts that occurred during match participation. Three measures of impact frequency were computed for each player: (1) player position impacts, the total and average number of head impacts recorded for the playing position for all matches; (2) player group impacts, the total and average number of recorded head impacts for the playing group (hit-up forwards, adjustables and outside backs) for all matches; and (3) impacts per match, the total and average number of impacts per match for all matches.
The head impact location variables were computed as azimuth and elevation angles relative to the centre of gravity (CG) of the head centered on the mid-sagittal plane.[37]These were categorized as front, side, back and top. Impacts to the top of the head were defined as all impacts above an α of 65° from a horizontal plane through the CG of the head. impacts were also assessed for tolerance[39,40] and impact severity,[41,42] Head Impact telemetry Severity profile (HITSP)[38]and Risk Weighted Exposure Combined Probability (RWECP).18 The HITSP is a weighted composite score including linear and rotational accelerations, impact duration, and impact location and the RWECP is a logistic regression equation and regression coefficient of injury risk prediction of an injury occurring based on previously published analytical risk functions. The RWECP combines the linear and rotational accelerations to elucidate individual player and team-based exposure to head impacts. As a value of 63 is a 75% indicator for a concussive injury[43] the HITSP values were evaluated by limits of less than 25% risk (< 21), 25% to 75% risk (21-63) and >75% risk (>63). The RWECP values were evaluated by the same values of 25% risk (< 0.2500) 25% to 75% risk (0.2500-0.7500) and >75% risk (>0.7500). The cumulative impact burden of the HITSP and RWECP values were calculated for every match over the duration of the study. Although there is no accepted method to quantify cumulative impact burden,[39] the sum of resultant PLA(g), PRA(rad/s2), HITSP and RWECP associated with each individual head impact per-match over the course of the study was calculated for all of these parameters.
3. Statistical Analysis
All filtered data on the Excel 2016 spreadsheet were analysed with SPSS V.24.0.0. The impact variables were not normally distributed (Kolmogorov-Smirnov; p< 0.001) therefore, data were expressed as mean (SD), median [IQR], and 95th percentile.[44,45] Additionally the cumulative impact burden per-match was analysed using a Kruskal-Wallis one-way ANOVA with a Dunn’s post-hoc test for all pair wise comparisons with player positions. Head impact exposure including impact duration, frequency, magnitude and location of impacts were quantified using previously established methods.[46]Median peak linear and rotational accelerations and impact locations between player positions were assessed using a Friedman repeated measures ANOVA on ranks with a Wilcoxon signed-rank test for post hoc analysis. Impact locations were analysed by front, back, side and top impacts using a Friedman repeated measures ANOVA on ranks by comparing impacts sustained in each location. A one sample chi-squared (χ2) test and risk ratio (RR) with 95% confidence intervals (CI) was used to determine whether the observed impact frequency was significantly different from the expected impact frequency. The HITSP and RWECP were analysed by total, forwards, outside backs and adjustables impacts using a Friedman repeated measures ANOVA on ranks. Post hoc analysis with Wilcoxon signed-rank tests was conducted with a Bonferroni correction applied. Statistical significance was set at p< 0.05.
4. Results
Thirty-one matches were completed over the study resulting in a match exposure of 536 match hours. A total of 20,837impacts to the head were recorded that were above the 10gdata acquisition threshold (see Table 1).The mean number of impacts to the head per-player over the season of matches was 672 ±237. This resulted in 52 ±79 impacts to the head per-player, per-match. Players recorded a median [IQR] of 14 [10 to 23] g for resultant PLA (g), and 3,181 [1,830 to 5,612] rad/s2for resultant PRA (rad/s2) over the duration of the study.
Over the study the hit-up forwards recorded more total impacts (n=9,464) than adjustables (n=6,627; p< 0.001) and outside backs (n=4,746; p< 0.001) (see Table 1). Hit-up forwards recorded a higher median PLA (g) (17 [12 to 26] g) than outside backs (13 [10 to 19] g;p< 0.001) and adjustables (12 [10 to 19] g;p< 0.001).
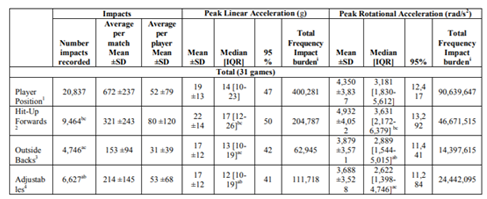
Adjustables recorded a lower median PRA (rad/s2) (2,622[1,398 to 4,746] rad/s2) than outside backs2, 889 [1,544 to 5,015] rad/s2; p< 0.001) and hit-up forwards (3,631[2,172 to 6,379] rad/s2; p< 0.001).
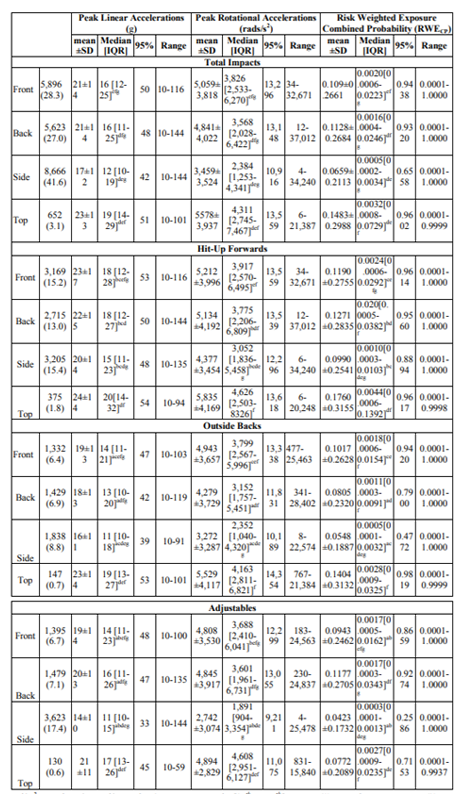
The side of the head was the most common impact location (n=8,666; 42%) compared with the front (n=5,896; 28%), back (n=5,623; 27%) or top (n=652; 3%) of the head. Hit up forwards recorded more impacts to the front of the head than outside backs (RR: 1.9 [95% CI: 1.1 to 1.3]; p< 0.0001) and adjustables (RR: 1.6 [95% CI: 1.5 to 1.7]; p< 0.0001) (see Table 2). Hit-up forwards (15 [11 to 23] g) recorded a higher median PLA (g) to the side of the head then outside backs (11 [10 to 18] g; p< 0.0001) and adjustables (11 [10 to 15] g; p< 0.0001) over the study. Hit-up forwards recorded a higher median PRA (rad/s2) (3,775 [2,206 to 6,809] rad/s2) than outside backs (3,152 [1,757 to 5,451] rad/s2; p=0.0046) and adjustables (3,601 [1,961 to 6,731] rad/s2; p=0.8966) to the back of the head. As a result, hit-up forwards recorded the highest median RWECP (0.0020[0.0005to 0.0382]) than outside backs (0.0011[0.0003to 0.0091]; p< 0.0001) and adjustables (0.0017 [0.0003 to 0.0343]; p< 0.0001) to the back of the head over the study.
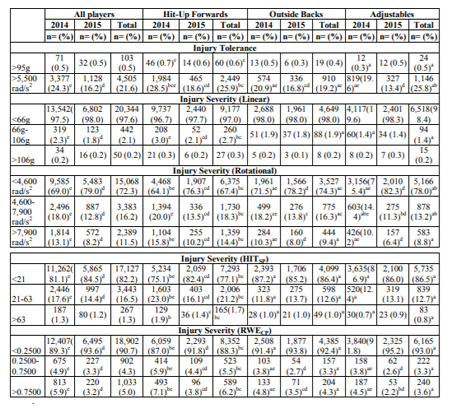
There were 103 impacts (0.5%) above the linear injury tolerance threshold and 4,505 impacts (22%) above the rotational injury tolerance threshold over the study (see Table 3). There were proportionally more impacts recorded above the linear injury tolerance threshold (>96 g) in the first, than the second year, of the study (24% vs. 16%; p< 0.001). Hit-up forwards recorded more impacts in the moderate PLA(g) (66g to 106g) in the first, than the second year, of the study (3% vs. 2%; p=0.0193). As a result, hit-up forwards recorded more moderate HITSP (21 to 63) (23% vs. 16%; p< 0.001) and RWECP (0.2500 to 0.7500) (6% vs. 4%; p=0.0040). Hit- up forwards (29%) recorded more impacts above the rotational injury threshold (>5,500 rad/s2) than outside backs (21%; p< 0.001) and adjustables (20%; p< 0.001) in the first year of the study. Adjustables (11%) recorded fewer impacts in the moderate (4,500 to 7,900 rad/s2) rotational injury severity threshold than hit-up forwards (14%; p=0.0287) and outside backs (14%; p=0.0174) in the second year of the study. Hit-up forwards recorded more severe HITSP (>63) (2%) and RWECP (>0.7500) (6%) when compared with outside backs (1%; p=0.0011: 4%; p< 0.0001) and adjustables (1%; p=0.00135: 4%; p< 0.0001) over the study.
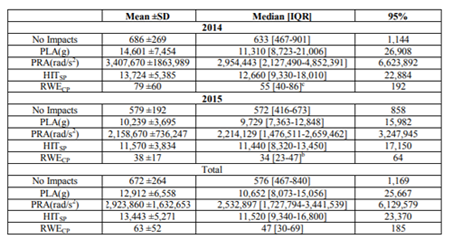
The total impact frequency burden per-match can be seen in Table 4. There was a median of 576 [467 to 840] impacts to the head per-match over the duration of the study. As a result, there was a median annual total impact frequency burden of 10,652 [8,073 to 15,056] g for linear accelerations,2,532,897[1,727,794to 3,441,539] rad/s2 for rotational accelerations; 11,520 [9,340 to 16,800] for HITSP and 47 [30 to 69] for RWECP per-match. The total impact frequency burden of the RWECP was higher in 2014 (55[40 to 86] than 2015 (34 [23 to 47]; p=0.0096) on post-hoc analysis.
Players received an average of 52 impacts to the head over 10g per game over the course of the study. As there are no published studies reporting impact biomechanics in rugby league the inter-study comparisons are limited to New Zealand senior amateur rugby union, American high-school and collegiate football studies. Not every study reviewed utilised the same reporting format, or data acquisition limit, necessitating the reporting of data as mean (±SD), median [25th-75 IQR] and 95th percentile at the 10g data acquisition limit. Even with using these reporting formats, some studies utilised the 75th percentile, the median of the 95th percentile,46 while other studies did not report rotational accelerations 13limiting inter-study comparisons. Some studies combined matches and practices and only reported the total biomechanical data while others incorporated both match and practice biomechanical data, 46again limiting potential comparisons. As shown in this study, there are a variety of magnitudes able to be reported and as we have provided mean (±SD), median [IQR] and 95th percentile this does make it complex to read but provides data for a wider inter-study analysis to be completed. A consensus34 needs to be established on what the reporting formats for impact biomechanical data (i.e. match vs practice and not combined) should be, and what parameters should be reported (i.e. PLA(g), PRA(rad/s2), HITsp, GSI, HIC15, RWECP) to enable future inter-study comparisons to be completed.
The median PLA(g) value recorded (14g) were similar to youth rugby union (15 g),30but lower than American youth (20.2 g, 22g),47, 48high school (21.7 g)18and collegiate (15g, 21g, 22g)13, 46, 49 football players and high school (30.9 g) and collegiate (31.9 g) soccer players. 24The mean PLA(g) (19g) was lower than the mean reported for American youth (25.5 g, 32g),48, 50and collegiate(21 g,),49 football players and New Zealand senior amateur rugby union (22g) players. 10The median PRA (rad/s2) value recorded (3,181rad/s2) was higher than the median (671 rad/s2; 1,013 rad/s2) but similar to the 95th percentile (2,743 rad/s2; 2,347 rad/s2) reported in American high school football.8, 18 When compared with American collegiate football, the median PRA(rad/s2)value recorded was higher than the median of impacts reported (1,392 rad/s2), 51sub concussive rotational accelerations (872-981 rad/s2),17but lower than the concussive PRA(rad/s2)recorded (4,948 rad/s2).17 When reviewed by the mean PRA(rad/s2) (4,350 rad/s2), this was higher than studies reporting data for American high school players(1,670 rad/s2)52but similar to New Zealand senior amateur rugby union10 players (3,990 rad/s2).When compared to the median of the 95th percentile of American collegiate football players (3,147 rad/s2)51 the findings were lower than the mean of the impacts recorded, but the 95th percentile of the peak rotational accelerations recorded in this study were higher (11,562 rad/s2). The higher extreme values could be reflective of the activities undertaken in rugby league when compared with American football and rugby union. Rugby league requires that players are tackled and taken to the ground after having a 10 m running gap between the defensive and attacking sides. The tackle typically requires two to three players wrestling the ball carrier to the ground with the focus to dominate the tackle, while the ball carrier tries to maintain an upright position in an effort for a fast play-the-ball. Further studies are warranted to identify the tackling differences between rugby league, rugby union and American football.
The distribution of impacts by location showed that 42% of impacts occurred to the side of the head which is in conflict with other studies reporting impacts in American high school (front of the head)7 and collegiate (top of the head)13, 51 football but similar to head impact position for New Zealand senior amateur rugby union.10 When viewed by positional groups the front of the head was the most common impact location for hit-up forwards (36%) which was similar for studies reporting American youth (43%)48 and collegiate (36%) 13 football impacts in games but different to that reported in senior amateur rugby union in New Zealand.10 The differences in the impact locations when viewed by positional groups are likely reflective of the roles these groups play during rugby league matches when compared with American football and senior amateur rugby union. Hit-up forwards are more involved in taking the ball straight into the opposition defensive line and are involved in more front on tackle situations and therefore recorded more impacts to the side and front of the head (15%).In contrast, the outside backs (side: 8.8%) and adjustable (side: 17.4%) are involved in wider roaming roles to either go outside the defensive line or to attack the defensive line on an angle with the aim of breaking through the line to score a try.
It has been suggested that concussions, or a combination of concussions and sub-concussive head impacts, may result in long-term conditions such as chronic traumatic encephalopathy,53 mild cognitive impairment54 and depression55 but the exact mechanisms that result in these conditions is not yet fully understood. Although cumulative impact burden is suspected to play a role in the development of these conditions,39 this has yet to be established.
The large number of impacts per-match, linear and rotational accelerations, HITSP and RWECP values recorded over the duration of this study may be an indicator of the possible risk these players may have for these long-term conditions. However, the data should in no way be interpreted as evidence to refute or support a cause-and-effect39 that these players may have, or will have, any of these conditions. The signs and symptoms of these conditions typically occur after players have ceased playing contact sports and currently cannot be attributed directly to the exposure to these impacts. This study only recorded impacts to the head from match activities and did not account for exposure to impacts in the training environment or through other activities of daily living that individual players may be exposed to.
6. Limitations
Data fromX2Biosystems XPatch accelerometers have been reported in previous studies,[56-58] of which two studies24, 25 tested the biomechanical validity in different settings. By comparing in-vivo performance of the XPatch via video capture in a simulated low-impact soccer setting, Wu et al.25 studied 25 impacts, one impact location, one mastoid placement location and one XPatch accelerometer on a single subject. It was reported25 that the XPatch over-estimated individual linear and rotational accelerations that was likely to be related to the subject’s viscoelastic properties of the soft tissues. In another study, McCuen et al.24 Evaluated the X Patch on a Hybrid III head form as a prelude to live-play soccer. There were 250 impacts over five impact locations with two mastoid placement locations and five different XPatch accelerometers. It was reported24 that there was significant XPatch measurement root mean square error related to individual impacts for PLA and PRA of ~50%. The study also looked at aggregate performance over a larger number of impacts and reported that the “average values over a large number of acceleration events can be determined with good accuracy."24 In another study utilising the XPatch in collegiate football, Reynolds et al.57 reported that the number and linear severity of head impacts were favorable comparable to published studies reporting[59,60]data for helmet based accelerometers. However, there were discrepancies reported[57] between the rotational severity of head impacts measured by the XPatch and similar published data from helmeted systems.[56] More recently Chrisman et al.36 evaluated the XPatch on a Hybrid III headform to a criterion standard and reported there was an over-estimation for PLA and an underestimation for PRA. As a result, they adjusted the XPatch results to the criterion standard. These adjustment calculations were therefore incorporated into the results of our study.
The use of the XPatch was novel in that the patch incorporates the accelerometer and gyroscope into a reusable monitor adhered to the side of the head behind the ear directly over the mastoid process of the player. The patches were applied utilising an adhesive patch to hold the patch to the adhesive and this was applied to the side of the head behind the ear. The effects of sweating by the player, and some extreme weather conditions, resulted in some of the adhesives falling off the player during the match activities. Players who were grabbed around the head during the tackle sometimes had the patch pulled off. As a result, the data reported were incomplete and the number of impacts would be more than have been reported. It is unlikely that the XPatch was tested under all of the activities seen in rugby league matches such as the tackle and scrum situations and how these correlate to the laboratory conditions results. Although we have reported these data, there are no consistent reliability studies for the XPatch and the interpretation of these results should be undertaken with some caution.
All games were captured on video to enable verification of the impacts recorded. The percentage of impacts that were able to be identified by video review and analysis was only 90% of the total impacts recorded per match, as only one video recorder was used. The ball carrier with possession of the ball is required to be tackled to the ground and, in most cases, this required two or more defenders to be involved in the tackle. The aim of the tackler was to stop the momentum of the ball carrier from gaining ground, or to cause the ball carrier to lose possession of the ball. Once momentum is stopped the objective is to take the ball carrier to the ground and, ideally, turned on their back to slow down the play-the-ball situation. Defending players joining the tackle in an attempt to put the ball carrier on the ground would result in multiple impacts to the ball carrier being recorded. As a result, not all the impacts recorded were able to be identified with the use of only one camera. This is a limitation of the study and future studies should include at least three high definition video cameras placed on one side of the field and one at each end of the playing field, preferably in an elevated position.
7. Conclusion
The study was conducted to describe the magnitude, frequency and distribution of head impacts sustained by a single amateur senior premier rugby league team over a competition season of matches. By utilising accelerometer fitted patches applied behind the ear of players in a single premier team throughout the 2014 and 2015 domestic seasons of matches there were 20,837 impacts recorded. Median linear accelerations were lower than high school and collegiate American football while the median rotational accelerations were higher. Further studies should further explore head impact characteristics at all levels of participation in rugby league.
References
- King D, Hume P, Milburn P, et al. Match and training injuries in rugby league: A review of published studies. Sports Med. 2010; 40(2):163-178.
- Gabbett T. Science of rugby league football: A review. J Sports Sci 2005; 23(9):961-976.
- Gibbs N. Injuries in professional rugby league. A three-year prospective study of the South Sydney professional rugby league football club. Am J Sports Med. 1993; 21(5):696-700.
- Gissane C, Jennings D, Kerr K, et al. A pooled data analysis of injury incidence in rugby league football. Sports Med. 2002; 32(3):211-216.
- King D, Hume P, Clark T. Video analysis of tackles in professional rugby league matches by player position, tackle height and tackle location. Int J Perform Anal Sport. 2010; 10(3):214-254.
- Wong R, Wong A, Bailes J. Frequency, magnitude, and distribution of head impacts in Pop Warner football: The cumulative burden. Clin Neurol Neurosur. 2014; 118:1-4.
- Broglio S, Sosnoff J, Shin S, et al. Head impacts during high school football: A biomechanical assessment. J Athl Train. 2009; 44(4):342-349.
- Daniel R, Rowson S, Duma S. Head impact exposure in youth football. Ann Biomed Eng. 2012; 40(4):976-981.
- Crisco J, Wilcox B, Beckwith J, et al. Head impact exposure in collegiate football players. J Biomech. 2011; 44(15):2673-2678.
- King D, Hume P, Brughelli M, et al. Instrumented mouthguard acceleration analyses for head impacts in amateur rugby union players over a season of matches. Am J Sports Med. 2015; 43(3):614-624.
- Talavage T, Nauman E, Breedlove E, et al. Functionally-detected cognitive impairment in high school football players without clinically-diagnosed concussion. J Neurotrauma. 2014; 31(4):327-338.
- Ng T, Bussone W, Duma S. The effect of gender and body size on linear accelerations of the head observed during daily activities. Biomed Sci Instrum. 2006; 42:25-30.
- Mihalik J, Bell D, Marshall S, et al. Measurements of head impacts in collegiate football players: An investigation of positional and event type differences. Neurosurgery. 2007; 61(6):1229-1235.
- Bailes J, Petraglia A, Omalu B, et al. Role of subconcussion in repetitive mild traumatic brain injury. J Neurosurg. 2013; 119(5):1235-1245.
- Spiotta A, Shin J, Bartsch A, et al. Subconcussive impact in sports: a new era of awareness. World Neurosurg. 2011; 75(2):175-178.
- Cobb B, Urban J, Davenport E, et al. Head impact exposure in youth football: Elementary school ages 9–12 years and the effect of practice structure. Ann Biomed Eng. 2013; 21(12):2463-2473.
- Rowson S, Duma S, Beckwith J, et al. Rotational head kinematics in football impacts: An injury risk function for concussion. Ann Biomed Eng. 2012; 40(1):1-13.
- Urban J, Davenport E, Golman A, et al. Head impact exposure in youth football: High school ages 14 to 18 years and cumulative impact analysis. Ann Biomed Eng. 2013; 41(12):2474-2487.
- Broglio S, Schnebel B, Sosnoff J, et al. Biomechanical properties of concussions in high school football. Med Sci Sports Exerc. 2010; 42(11):2064-2071.
- Eckner J, Sabin M, Kutcher J, et al. No evidence for a cumulative impact effect on concussion injury threshold. J Neurotrauma. 2011; 28(10):2079-2090.
- Hanlon E, Bir C. Real-time head acceleration measurements in girls youth soccer. Med Sci Sports Exerc. 2012; 44(6):1102-1108.
- Pellman E, Viano D, Tucker A, et al. Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery. 2003; 53(4):799-814.
- Zhang L, Yang J, King A. A proposed injury threshold for mild traumatic brain injury. J Biomed Eng. 2004; 126(2):226-236.
- McCuen E, Svaldi D, Breedlove K, et al. Collegiate women's soccer players suffer greater cumulative head impacts than their high school counterparts. J Biomech. 2015; 48(13):3720-3723.
- Wu L, Nangia V, Bui K, et al. In vivo evaluation of wearable head impact sensors. Ann Biomed Eng. 2015; 44(4):1234-1245.
- Wilcox BJ, Beckwith JG, Greenwald RM, et al. Biomechanics of head impacts associated with diagnosed concussion in female collegiate ice hockey players. J Biomech. 2015; 48(10):2201-2204.
- Wilcox B, Machan J, Beckwith J, et al. Head-impact mechanisms in men's and women's collegiate ice hockey. J Ath Train. 2014; 49(4):514-520.
- Wilcox B, Beckwith J, Greenwald R, et al. Head impact exposure in male and female collegiate ice hockey players. J Biomech. 2013; 47(1):109-114.
- Broglio S, Eckner J, Kutcher J. Field-based measures of head impacts in high school athletes. Curr Opin Pediatr. 2012; 24(6):702-708.
- King D, Hume P, Gissane C, et al. Similar head impact acceleration measured using instrumented ear patches in a junior rugby union team during matches in comparison with other sports. J Neurosurg Pediatr. 2016; 18(1):65-72.
- King D, Hume P, Gissane C, et al. Head impacts in a junior rugby league team measured with a wireless head impact sensor: An exploratory analysis. J Neurosurg Pediatr. 2016; 19(1):13-23.
- King DA, Hume PA, Gissane C, et al. Head impact exposure from match participation in women's rugby league over one season of domestic competition. J Sci Med Sport. 2017; doi: 10.1016/j.jsams.2017.10.026.
- Gabbett T, Kelly J, Pezet T. A comparison of fitness and skill among playing positions in sub-elite rugby league players. J Sci Med Sport. 2008; 11(6):585-592.
- King D, Hume P, Gissane C, et al. The influence of head impact threshold for reporting data in contact and collision sports: Systematic review and original data analysis. Sports Med. 2016; 46(2):151-169.
- Mihalik J, Blackburn J, Greenwald B, et al. Collision type and player anticipation affect head impact severity among youth ice hockey players. Pediatrics. 2010; 125(6):e1394-e1401.
- Chrisman S, Mac Donald C, Friedman S, et al. Head impact exposure during a weekend youth soccer tournament. J Child Neurol. 2016; 31(8):971-978.
- Crisco J, Chu J, Greenwald R. An algorithm for estimating acceleration magnitude and impact location using multiple nonorthogonal single-axis accelerometers. J Biomech Eng. 2004; 126(6):849-854.
- Greenwald R, Gwin J, Chu J, et al. Head impact severity measures for evaluating mild traumatic brain injury risk exposure. Neurosurgery. 2008; 62(4):789-798.
- Broglio SP, Eckner J, Martini D, et al. Cumulative head impact burden in high school football. J Neurotrauma. 2011; 28(10):2069-2078.
- Guskiewicz K, Mihalik J, Shankar V, et al. Measurement of head impacts in collegiate football players: relationship between head impact biomechanics and acute clinical outcome after concussion. Neurosurgery. 2007; 61(6):1244-1253.
- Harpham J, Mihalik J, Littleton A, et al. The effect of visual and sensory performance on head impact biomechanics in college football players. Ann Biomed Eng. 2013; DOI: 10.1007/s10439-013-0881-8.
- Ocwieja K, Mihalik J, Marshall S, et al. The effect of play type and collision closing distance on head impact biomechanics. Ann Biomed Eng. 2012; 40(1):90-96.
- Broglio S, Eckner J, Surma T, et al. Post- concussion cognitive declines and symptomatology are not related to concussion biomechanics in high school football players. J Neurotrauma. 2011; 28(10):2061-2068.
- Hopkins W, Marshall S, Batterham A, et al. Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc. 2009; 41(1):3-12.
- Hopkins W, Marshall S, Quarrie K, et al. Risk factors and risk statistics for sports injuries. Clin J Sports Med. 2007; 17(3):208-210.
- Crisco J, Fiore R, Beckwith J, et al. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train. 2010; 45(6):459-559.
- Daniel R, Rowson S, Duma S. Head impact exposure in youth football: Middle school ages 12-14 years. J Biomech Eng. 2014; 136(9):094501-094506.
- Munce T, Dorman J, Thompson P, et al. Head impact exposure and neurologic function of youth football players. Med Sci Sport Exerc. 2015; 47(8):1567-1576.
- Brolinson P, Manoogian S, McNeely D, et al. Analysis of linear head accelerations from collegiate football impacts. Curr Sports Med Rep. 2006; 5(1):23-28.
- Duma S, Manoogian S, Bussone W, et al. Analysis of real-time head accelerations in collegiate football players. Clin J Sport Med. 2005; 15(1):3-8.
- Crisco J, Wilcox B, Machan J, et al. Magnitude of head impact exposures in individual collegiate football players. J Appl Biomech. 2012; 28(2):174-183.
- Broglio S, Surma T, Ashton-Miller J. High school and collegiate football athlete concussions: A biomechanical review. Ann Biomed Eng. 2012; 40(1):37-46.
- Gavett B, Stern R, McKee A. Chronic traumatic encephalopathy: A potential late effect of sport-related concussive and subconcussive head trauma. Clin Sports Med. 2011; 30(1):179-188.
- Guskiewicz K, Marshall S, Bailes J, et al. Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery. 2005; 57(4):719-726.
- Guskiewicz K, Marshall S, Bailes J, et al. Recurrent concussion and risk of depression in retired professional football players. Med Sci Sports Exerc. 2007; 39(6):903-909.
- Reynolds BB, Patrie J, Henry EJ, et al. Practice type effects on head impact in collegiate football. J Neurosurg. 2016; 124(2):501-510.
- Reynolds B, Patrie J, Henry E, et al. quantifying head impacts in collegiate lacrosse. Am J Sports Med. 2016; doi: 10.1177/0363546516648442.
- Swartz EE, Broglio SP, Cook SB, et al. Early results of a helmetless-tackling intervention to decrease head impacts in football players. J Ath Train. 2015; 50(12):1219-1222.
- Rowson S, Brolinson G, Goforth M, et al. Linear and angular head acceleration measurements in collegiate football. J Biomed Eng. 2009; 131(061016):1-7.
- Schnebel B, Gwin J, Anderson S, et al. In vivo study of head impacts in football: A comparison of National Collegiate Athletic Association division I versus high school impacts. Neurosurgery. 2007; 60(3):490-496