


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
CT Signs of Diffuse Idiopathic Skeletal Hyperostosis (DISH)
Suheil Artul1,2*, William Nseir2,3, Najib Nasralla3, Faozi Artoul4, marron daud1, George s. Habib3
2.Faculty Medicine in the Galilee, Bar-Ilan University, Safed Israel.
3.Department of Medicine, Nazareth Hospital
4.Nuclear medicine, Meir Hospital, Israel
Copyright : © 2017 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Diffuse idiopathic skeletal hyperostosis (DISH) is considered an underdiagnosed and mostly asymptomatic non-inflammatory osteoarthritis. The etiology of DISH remains unknown with no validated diagnostic criteria. This condition is solely diagnosed radiologically. Symptoms vary from asymptomatic to disabling neurological conditions. In this paper we report a case of progressive dysphagia and neck pain due to DISH of the cervical spine in a 73-year-old man, imaging studies was used to support the diagnosis.In this paper, we also discuss the clinical features and differential diagnosis and review of literature.
1. Introduction
Jacques Forestier and his student Jaume Rotes-Querol described the entity as “senile ankylosing vertebral hyperostosis” back in the 50’s as Forestier disease. Later on, Resnick and Niwayama coined the term “diffuse idiopathic skeletal hyperostosis” (DISH) which is still cur-rently in use.
2. Case Presentation
A 73 year old man presented to our institution with progressive dysphagia and neck stiffness. Despite progressive conventional treatment, there was no relief whatsoever. The dysphagia was more for solid than for liquid. The patient didn’t have other complains such as weight loss. The patient is healthy otherwise.
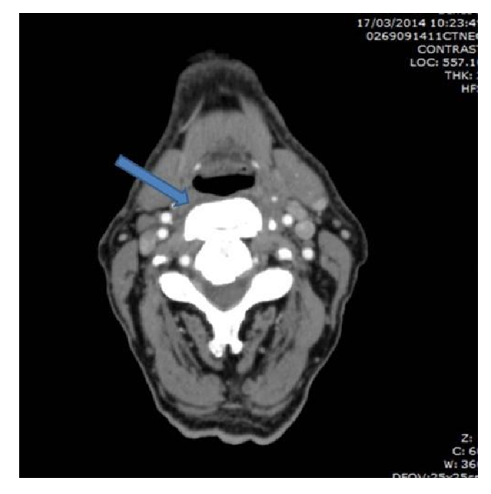
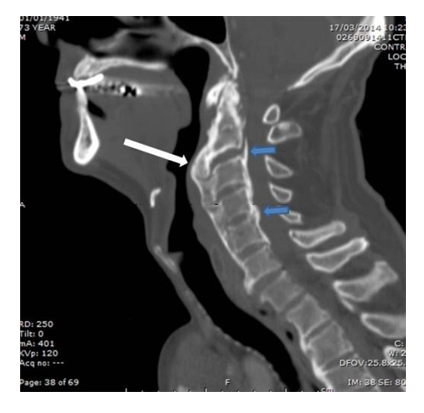
A detailed clinical examination which included a direct pharyngoscope has revealed a bulging mass that compresses the oropharyngeal space. Further investigation with CT study of the neck has rule out the existence of a real mass, instead revealed a huge anterior osteophyte bridging between C2-C3, bulging to the oropharynx with preservation of the intervertebral spaces and ossification of the posterior longitudinal ligament (figure 1+2), features consisting with the diagnosis of DISH. Surgical treatment was rec-ommended, however the patient refused.
3. Differential Diagnosis
A wide spectrum of medical condition overlaps with DISH. Ankylosing spondylitis (AS) sprung up a major concern differentiating it from DISH both clinically and radiologically; both entities cause a certain degree of spinal deformability and postural abnormality and both share the in-volvement of axial skeleton and peripheral enthesis. Clinically, AS present at an earlier stage of life, mainly consist of inflammatory spinal pain and stiffness leading to a decreased range of spinal movement. Advanced AS pre-sents characteristically with postural abnormali-ty, notably Bechterew stoop. On the other hand, DISH affect primarily middle-aged person and it is often asymptomatic in presentation or with mild spinal pain. Radiologically, AS typically presents with bilateral symmetrical erosivesacroiliitis, Romanus lesion and squaring of the vertebral bodies leading to bamboo spine,which consists of bilateral marginal para-vertebral symmetrical syndosmphytes that radiologically differ from osteophyte by the fact that is vertically oriented rather than horizontal such as the osteophyte.
Degenerative osteoarthritis (OA) is considered one of the most common chronic conditions af-fecting the joints, and one of the most common causes of osteophyte formation in the cervical spine. OA is, however, readily differentiated from DISH giving its distinguished radiological appearances such as disk space narrowing, scle-rosis. These patterns are less frequently seen in DISH.
Other conditions that should be taken into con-sideration are Psoriatic arthritis, Reactive arthri-tis and retinoid arthropathy.
4. Discussion
Diffuse Idiopathic skeletal hypertosis is often considered underdiagnosed or misdiagnosed with other medical condition attributed to diffi-culties recognizing its’ radiological features, as It is diagnosed primarily based on a specific set of radiological characteristics.
Its etiology remains nowadays unknown, how-ever several authors speculate an involvement of several elements such as mechanical factors, genetic factors (HLA genes), environmental ex-posures (fluoride, vitamin A/retinol), drugs (isotretinoin, etretinate, acitretin and other vita-min A derivatives), and metabolic conditions have been hypothesized to be part of ethiopathogenesis [1].
Epidemiologically, it kicks off in middle aged men and elderly persons, with predilection to men predominance. The prevalence of DISH increases with age, as Holton et al. estimated 40% in a population of more than 65 years of age [2].
Clinically, DISH can present with variable spectrum from totally asymptomatic to a rarely cata-strophic neurological complication. In most cas-es, DISH patients are utterly asymptomatic and it is often accidentally found by radiographs of the spine performed due to a decreased range of motion of spinal joints and enthesis-related pain [2,3]. Symptomatic patients often present with neck pain or progressive dysphagia. According to a meta-analysis by Dutta et al [4], only 73 cases of Forestier disease presenting with dysphagia were reported till 2010 in the English literature. Dysphagia results when the cervical spine is involved with prevalence rate of 17-28% [5]. Bony projections can rarely cause intraspinal compressive neurological symptoms [6].
DISH primarily affect spinal skeletal, it is characterize by flowing mantle ossification and calcification of the anterior and posterior longitudinal ligaments. Other spinal areas could be affected as well to a lesser extent such as the paravertebral connective tissue and the periphery of the annulus fibrosus. Such deformity can affect any part of the skeletal spine, however the thoracic spine is the most affected segment followed by lumbar and cervical respectively in descending frequency. Notably it may affect more than one segment simultaneously.
DISH nowadays is still diagnosed radiologically. Several set of criteria were used to this aim. The classification most commonly used for DISH was proposed by Resnick and Niwayama [6,7] which required flowing anterol-ateral ossification of at least four contiguous thoracic vertebral segments, preservation of the intervertebral disc spaces and absence of apophyseal joint degeneration or sacroiliac inflammatory changes.
5. Conclusion
In summary, DISH is a diverse underdiagnosed and misdiagnosed disease with an increasing prevalence above the age of 65. It is commonly affecting the spinal skeletal with consequent ossification and calcification of the anterior and posterior longitudinal ligaments with variable involvement of other spinal structures. Dysphagia is the most common presenting feature when the cervical spine is involved. Other symptoms include neck pain and reduced neck mobility. The radiological features of DISH are challeng-ing and require an expert differentiating them from entities mimicking this condition. The sole definitive treatment of dish remains surgi-cal removal of the osteophytes.
References
- Mader R, Verlaan JJ, Buskila D. Diffuse idio-pathic skeletal hyperostosis: clinical features and pathogenic mechanisms. Nat Rev Rheumatol. 2013; 9(12): 741–750
- Holton KF, Denard PJ, Yoo JU, Kado DM, Barrett-Connor E, Marshall LM. Osteoporotic Fractures in Men (MrOS) Study Group Diffuse idiopathic skeletal hyperostosis and its relation to back pain among older men: The MrOS study. Semin Arthritis Rheum. 2011; 41(2): 131–8.
- Childs SG. Diffuse idiopathic skeletal hyperos-tosis: Forestier’s disease. OrthopNurs. 2004; 23(6): 375–382.
- Presutti L, Alicandri-Ciufelli M, Piccinini A, et al. Forestier disease: single-center surgical ex-perience and brief literature review. Ann OtolRhinolLaryngol. 2010; 119(9):602–608.
- Dutta S, Biswas KD, Mukherjee A, Basu A, Das S, Sen I, et al. Dysphagia Due to Forestier Disease: Three Cases and Systematic Literature Review. Indian Journal of Otolaryngology and Head and Neck Surgery. 2014; 66 (Suppl 1): 379–84.
- Kos MP, Van Royen BJ, David EF, Mahieu HF. Anterior cervical osteophytes resulting in severe dysphagia and aspiration: two case re-ports and literature review. J Laryngol Otol. 2009;123(10):1169–73.
- Resnick D, Niwayama D. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH), radiology, 1976, vol.119 (pg. 559-68)