


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Extraosseous Aneurysmal Bone Cyst of the Ankle
Salem Bouomrani1*,2, Moez Ben Ayed2,3, Safa Trabelsi1, Nesrine Belgacem1
2.Sfax Faculty of Medicine. University of Sfax. Sfax 3029. Tunisia.
3.Department of Orthopedics. Regional Hospital of Gabes. Gabes 6000. Tunisia
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction: Extraosseous aneurysmal bone cyst (ACB) represents an exceptional and extremely rare variant of aneurysmal bone cysts. This presentation deserves to be known by clinicians and radiologists to avoid diagnostic delays.
We present an original case of extraosseous ABC arising in the soft tissues of the ankle.
Case report: A 16-year-old patient, without pathological medical history, was explored for a discomfort of the left foot when wearing shoes, painless and progressive swelling of the left ankle that has been evolving for two months. The standard X-ray of the ankle and ultrasound of the soft parts of the ankle were suggestive of myositis ossificans. The patient was operated with a complete curettage and spongy graft. The histological examination confirmed the diagnosis of ABC of soft tissues. The evolution was favorable.
Conclusion: The localization in the soft parts of the ankle of these benign bone tumors has not been reported before. Our observation is, to our knowledge, the first reporting this location.
Extraosseous aneurysmal bone cyst, aneurysmal bone cyst, ankle, soft tissues,Orthopedics
1. Introduction
The aneurysmal bone cyst (ABC) is a relatively recent nosological entity of individualization, since its first description dates back to 1942 by Jaffe HL and Lichtenstein L [1]. It has since been recognized and defined by the “Histopathological Classification of Primary Bone Tumors” of the World Health Organization (WHO) initially established in 1972 and revised in 1993, as "a benign, expansive osteolytic lesion, occurring most often in the metaphysis of long bones, vertebrae and flat bones, consisting of multiple hematological gaps separated by connective septa containing osteoclasts and reactive osteogenesis"; ABC is thus considered as a "tumor-like" lesion (group IX of primary bone tumors according to the WHO classification" [2]. It can be primitive in 70% of cases, developing in anteriorly normal bone, or secondary in 30% of cases emerging from other benign or malignant bone lesions [3-5].
It is a rare tumor representing only 1-2% of all bone tumors and about 10% of benign bone tumors [6]. Its incidence is estimated at 0.14 to 0.32/100,000/year, and is particularly common before the age of 20 and in female patients [4-6].
Beside classical ABC, atypical and unusual forms of this tumor (solid ABC and extraosseous or soft tissue ABC) can be seen and represent a real diagnostic challenge for clinicians [5].
We report an original observation of extraosseous ABC arising in the soft tissues of the ankle; location not previously reported in the English medical literature.
2. Case Report
A 16-year-old patient, without pathological medical history, was explored for a discomfort of the left foot when wearing shoes, painless and progressive swelling of the left ankle that has been evolving for two months. No concept of recent trauma or old fracture has been reported.
The somatic examination noted a deformed left ankle with subcutaneous swelling, hard, painless, non-mobile, and opposite the medial face of the calcaneus. The ankle joint was supple, painless at mobilization, and with preserved area of mobility.
Apart from this swelling, the somatic examination was without abnormalities as well as the basic biological assessment: total blood count, erythrocyte sedimentation rate, C-reactive protein, serum calcium, phosphoremia, alkaline phosphatase, creatinine, fasting glucose, uric acid, ionogram, transaminases, muscle enzymes, lactate dehydrogenase, and electrophoresis of serum proteins.
The standard X-ray of the ankle showed an extra-osseous opacity, rounded, well limited by a thin bone shell, containing some bony trabeculae inside, located opposite the medial face of the calcaneus, and measuring about 3 cm diameter (Figure 1). No associated lytic bone lesions were noted.
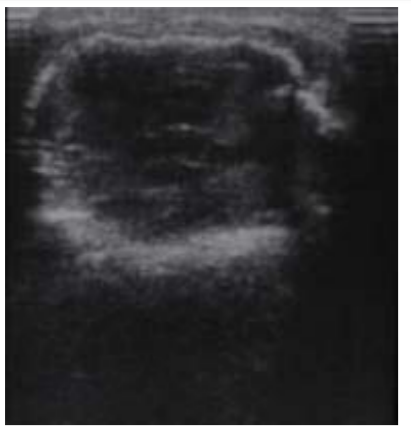
Ultrasound of the soft parts of the ankle revealed a hypoechoic mass, encapsulated by a hyperechoic shell, developing in the soft parts opposite the medial aspect of the calcaneus, and which does not seem to adhere to the cortical bone of the latter (Figure 2).
The patient was transferred to the department of orthopedic surgery with the diagnosis of myositis ossificans. The procedure consisted of a complete curettage with spongy graft. The postoperative course was simple.
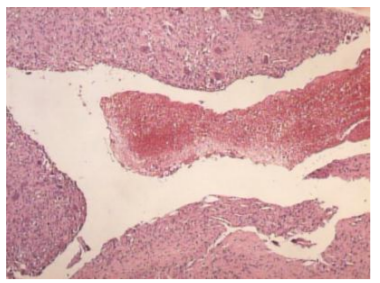
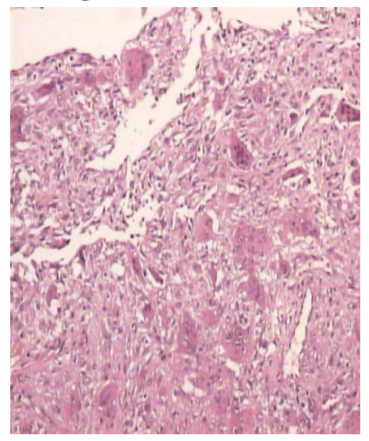
Anatomopathological examination of the operative specimen showed macroscopically the presence of multiple rounded hemorrhagic gaps separated from each other by connective septa. Microscopically, cavities were filled with blood and without endothelial lining (Figure 3), septa lined with fibroblasts, osteoclastic giant cells, and reactive bone tissue lined by osteoblasts (Figure 4). The electron microscopy study confirmed the presence of cells containing peripheral filaments suggesting their myofibroblastic differentiation. The histological aspect was compatible with the diagnosis of ABC in its extraosseous form.

3. Discussion
The soft tissues of the foot and ankle are generally unusual sites for the development of both benign and malignant primary tumors [7]. Cystic bone lesions are particularly rare in these soft tissues [8]. Of all these tumors, the ABC remains exceptional[7,8].
Extraosseous or soft tissues ABC is an extremely rare variant of ABC [5,9,10]. His first description goes back to Salm R and Sissons HA in 1972 [11], and was long confused with giant cell tumor of soft tissue [12] or myositis ossificans[13]. Since then only sporadic cases have been reported in the literature [9,10,14-17]; in fact, Lopez LV et al's review of English-language literature in 2017 found only 26 cases [9].
These forms of ABC are still unknown by health practitioners explaining the often significant diagnostic delay and often inadequate management [8,14]. They represent a real diagnostic challenge for both clinicians and radiologists [9].
These soft tissue ABCs can be seen at any age and in both sexes; the most frequent locations are the soft tissues of the lower limbs, arms, and shoulders [9,17]. The ankle remains an exceptional and unusual location; in fact, no case of extraosseous ABC of the ankle has been found in the literature according to the 2017 review by Lopez LV et al [9].
The clinic is classically reduced to soft tissue pain and tumefaction, sometimes with palpation of an expansive mass [4]. Standard radiography may paradoxically remain normal [15]. Ultrasound and nuclear magnetic resonance imaging will be of great diagnostic value in these situations [4,5,15]. The diagnosis of certainty remains histological [7,9,16,17]. The treatment of choice for these particular forms remains surgical excision and the evolution is usually favorable [7,9,16,17].
4. Conclusion
Soft tissue ACB or extraosseous ACB represents an exceptional and extremely rare variant of aneurysmal bone cysts. This presentation deserves to be known by clinicians and radiologists to avoid diagnostic delays. The localization in the soft parts of the ankle of these benign bone tumors has not been reported before. Our observation is, to our knowledge, the first reporting this location.
References
- Jaffe HL, Lichtenstein L: Solitary unicameral bone cyst: With emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg 1942;44:1004-1025.
- Schajowicz F, Sissons HA, Sobin LH. The World Health Organization's histologic classification of bone tumors. A commentary on the second edition. Cancer. 1995; 75(5):1208-14.
- Kransdorf MJ, Sweet DE. Aneurysmal bone cyst: concept controversy clinical presentation and imaging. Am J Roentgenol. 1995; 164(3):573-580.
- Rapp TB, Ward JP, Alaia MJ. Aneurysmal bone cyst. J Am Acad Orthop Surg. 2012;20(4):233-41.
- Mascard E, Gomez-Brouchet A, Lambot K. Bone cysts: unicameral and aneurysmal bone cyst. Orthop Traumatol Surg Res. 2015;101(1 Suppl): S119-27.
- Freiberg AA, Loder RT, Heidelberger KP, Hensinger RN. Aneurysmal bone cysts in young children. J Pediatr Orthop. 1994;14(1):86-91.
- Walling AK, Gasser SI. Soft-tissue and bone tumors about the foot and ankle. Clin Sports Med. 1994;13(4):909-38.
- Reda B. Cystic bone tumors of the foot and ankle. J Surg Oncol. 2018;117(8):1786-1798.
- Lopez LV, Rodriguez MG, Siegal GP, Wei S. Extraskeletal aneurysmal bone cyst: Report of a case and review of the literature. Pathol Res Pract. 2017;213(11):1445-1449.
- Baker KS, Gould ES, Patel HB, Hwang SJ. Soft tissue aneurysmal bone cyst: a rare case in a middle aged patient. J Radiol Case Rep. 2015;9(1):26-35.
- Salm R, Sissons HA. Giant-cell tumours of soft tissues. J Pathol. 1972;107:27-39.
- An SB, Choi JA, Chung JH, Oh JH, Kang HS. Giant cell tumor of soft tissue: a case with atypical US and MRI findings. Korean J Radiol. 2008;9:462-5.
- Amir G, Mogle P, Sucher E. Case report 729. Myositis ossificans and aneurysmal bone cyst. Skeletal Radiol. 1992;21:257-9.
- Wang XL, Gielen JL, Salgado R, Delrue F, De Schepper AM. Soft tissue aneurysmal bone cyst. Skeletal Radiol. 2004;33(8):477-80.
- Ajilogba KA, Kaur H, Duncan R, McFarlane JH, Watt AJ. Extraosseous aneurysmal bone cyst in a 12-year-old girl. Pediatr Radiol. 2005;35(12):1240-2.
- Rodríguez-Peralto JL, López-Barea F, Sánchez-Herrera S, Atienza M. Primary aneurysmal cyst of soft tissues (extraosseous aneurysmal cyst). Am J Surg Pathol. 1994;18(6):632-6.
- Riccioni L, Foschini MP. Extraosseous aneurysmal bone cyst. Tumori. 1996;82(5):485-7.