


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Safe Surgical Dislocation Approach for Open Reduction Internal Fixation of Femoral Head Fractures
Dr. Mohammed Hefnawy1*,Hossam Fekry1,Mohammed A Sebae1
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: In there are femoral head fractures, the majority of these injuries should be treated operatively and the choice of surgical approach and procedure was not settled. Surgical decision and reconstructive options are influenced by patient condition and fracture types.
Patients and Methods: Twenty patients with displaced femoral head fractures were surgically treated (ORIF) using surgical dislocation approach selectively. Minimum follow up was 30 months (mean, 48 months; SD, 30.6 months). According to Pipkin classification, we had displaced Type I in 8 hips, type II in ten hips. CT scan evaluation for all patients was done routinely. Radiological evaluation was done according to Matta’s criteria. The heterotopic ossification was graded according to the Brooker classification. Radiographs taken at the last follow up were evaluated and classified according to the Tönnis classification. Clinically, the patients were evaluated with the modified Harris hip score.
Results: The mean modified Harris hip score (HHS) was 84 points (range: 72-92) (SD, 7). Radiographically, fracture reduction was anatomic in fourteen hips and imperfect in four with a mean residual fracture displacement of 1.2 mm (SD, 1.65). AVN of the femoral head was found in one patient and underwent THA at 2 years. Two patients developed adventitious bursa on greater trochanter region and excision of trochanteric screws was done and improved. Heterotopic ossification grade I was recorded in three patients in this study until the final follow up but did not affect the function.
Conclusion: This technique is recommend for surgeons treating fracture femoral head with or without acetabular fractures as it provide full exposure of the femoral head. As a limitation of this study, the small number of cases and lake of previous studies using the same technique for the same indication. Future studies are required to compare this approach with others regarding the outcome scores and complications.
Safe, dislocation, internal fixation, femoral head, fractures,Orthopedics
1. Introduction
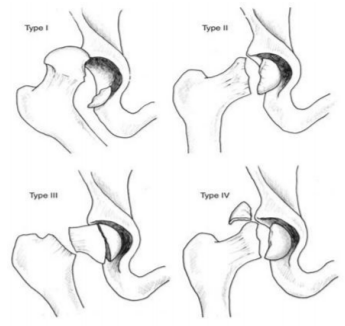
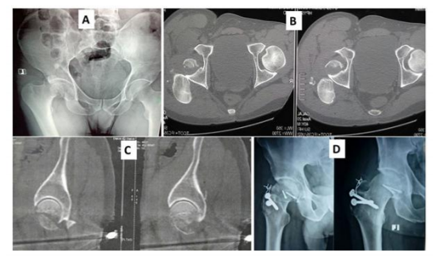
As the fractures of femoral head are rare, absolute recommendations for surgical management are difficult to make [1-3]. The choice of surgical approach and procedure was not settled. The majority of these injuries should be treated operatively. Surgical decision and reconstructive options are influenced by patient condition and fracture types [4]. Age of the patient, level of activity, bone quality, and associated comorbidities are important factors [5,6]. Pipkin classification type II, III, and IV fractures indicated for open reduction and internal fixation in young, active patients [7], but Pipkin type I fractures with displaced fragment treated according to its size and position either excision or fixation (Figure 1) [8].
Many approaches were used as anterior, posterior, and transtrochanteric surgical approaches, but the limited exposure is reported. Few studies have reported on the results using approaches that provide full exposure of the femoral head but spare the blood supply to the femoral head . This approach was utilized for treatment of other indications, including femoro-acetabular impingement, slipped capital epiphysis [9], and isolated acetabular fractures [10]. Concomitant acetabular fixation was performed in Type IV fractures.
The aim of this study is evaluation of the results of surgical hip dislocation for open reduction internal fixation (ORIF) of displaced femoral head fractures as regard the surgical technique, quality of fracture reduction; function, and complications.
2. Patients And Methods
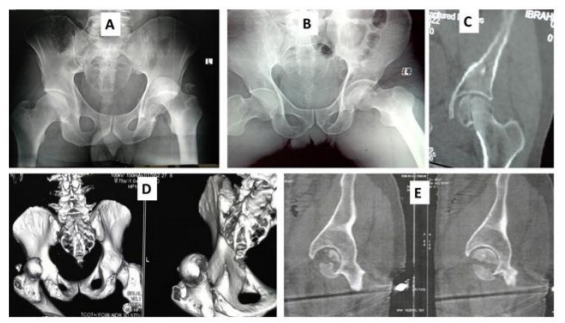
Between 2010 and 2016, twenty patients who presented with displaced femoral head fractures were surgically treated (ORIF) using surgical dislocation approach selectively. Minimum follow up was 30 months (mean, 48 months; SD, 30.6 months). According to Pipkin classification, we had displaced Type I in 8 hips, type II in tenhips, and two were lost during follow up. CT scan evaluation for all patients was done routinely (Figure 2). The mean surgical time was 100 minutes (SD, 32) ranged from 90-150 not including anesthetic time. The mean blood loss was 1100 mL (SD, 523) in the isolated femoral head fractures.
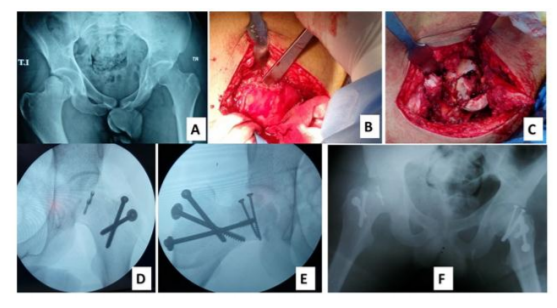
Lateral decubitus position was used in all cases. Gibson posterolateral incision was used to preserve more of the gluteus maximus muscle. Trochanteric osteotomy was done in all patients, with maintaining the insertion of the gluteus medius, vastus lateralis, and long tendon of the gluteus minimus muscles attached to the osteotomized fragment. Through the interval between the gluteus minimus and the piriformis muscles which is safe of damage to the deep branch of the medial circumflex artery.
The osteotomized trochanteric fragment wasslide anteriorly after releasing the origin of the gluteus minimus. T-shaped capsulotomy was done if the capsule was intact (8 cases) or completed when partial capsular rupture is present. Dislocation of the femoral head was then made and the acetabulum was inspected for loose fragments. To reduce the risk of avascular necrosis (AVN), a careful section of the ligamentum teres was performed in Type I fracture with curved scissors when the inferior fragment still attached to the ligamentum teres. For fixation of the femoral head fracture, we used Herbert screws under direct vision with or without added navicular 4 mm lag screws with avoidance of weight bearing zones and screw protrusion. Femoral head was then reduced within the acetabulum and fixed the trochanteric fragment with two or three 6.5 cancellous screws (Figure. 3).
Intraoperative findings: lack of congruence was found in 6 patients due to loss of small comminuted unfixable fragments of the head. All patients had intact Weitbrecht ligamentum; a labral tear was found in two patients which was repaired with the capsule after fixation. Multiple small fragments not fixable were found in six hips. Anterior impaction of the head was recorded in eight hips and bone loss (defined as a partial incongruence between femoral head fragments) was intraoperatively reported in 3 hips.
Radiological evaluation of the reduction of the fracture was done according to Matta’s criteria [11] measuring the residual displacements on the plain radiographs in millimeters: and classified as anatomical (0–1 mm of displacement), imperfect (2–3 mm), or poor (more than 3 mm). The heterotopic ossification was graded according to the Brooker classification [12]. Radiographs taken at the last follow up were evaluated and classified according to the Tönnis classification [13]. Clinically, the patients were evaluated with the modified Harris hip score [14].
3. Results
The mean modified Harris hip score (HHS) was 84 points (range: 72-92) (SD, 7) postoperatively in comparison to preoperative mean of 45 (range: 42-68). Excellent results (defined as a modified Harris hip score higher than 80 points) were achieved in 12 of the 18 patients; four good, two fair and no poor results were recorded.
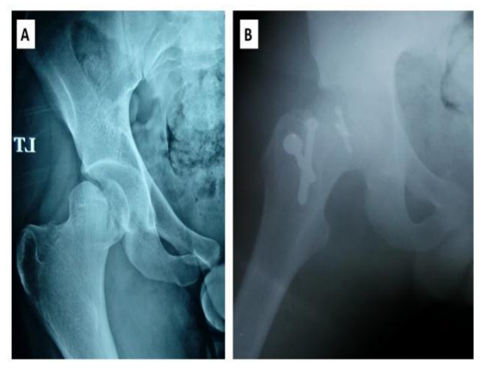
Radiographically, fracture reduction was anatomic in fourteen hips and imperfect in four with a mean residual fracture displacement of 1.2 mm (SD, 1.65) (Figure 4). AVN of the femoral head was found in one patient and underwent THA at 2 years. Two patients developed adventitious bursa on greater trochanter region and excision of trochanteric screws was done and improved.
Heterotopic ossification grade I was recorded in three patients in this study until the final follow up but did not affect the function. At the last follow up Tönnis classification was found as Grade I in four patients, Grade IIIin one patient who underwent arthroplasty, but all remaining patients were classified as Grade 0.
4. Discussion
Femoral head fractures are rare injuries, but the general consensus is that operative fixation is warranted. However, controversy exists about the choice of surgical approach for femoral head fractures. Anterolateral (Watson-Jones), anterior (Smith-Petersen), and posterolateral (Kocher-Langenbeck) approaches are the most used in the literature . The exposure is limited with classical approaches. Few studies have reported on the results using approaches such as surgical dislocation that provide full exposure of the femoral head but spare the blood supply to the femoral head [15].
The modified Harris hip score was used in this study. Other scores such as the Hip disability and Osteoarthritis Outcome Score were used in literatures. However, we used the Harris hip score here because it is familiar. For radiologic evaluation of reduction of the fracture, we used the Matta classification which has been described to evaluate acetabular fracture and shows a good correlation with posttraumatic arthritis development but has not used for femoral head fractures or posttraumatic arthritis. Few series are available in the literature for direct comparison as the femoral head fracture is rare. In addition, clinical outcomes are reported with a variety of scoring instruments. Henle et al. [16] reported on 12 patients using the Merle d’Aubigne and Postel scorefor clinical evaluation of their patients [17]. At 31.1 months, 10 patients had good outcomes and two were considered poor. Similarly, at 47 months, Solberg et al. [18] using the Merle d’Aubigne and Postel score reported on 12 patients with Pipkin IV fractures and noted good or excellent scores in 10 patients. These results are comparable to ours.
In a systematic review of 26 papers reporting on 405 femoral head fractures, Giannoudis et al. reported that clinical outcomes, defined as good or excellent results according to Thompson-Epstein criteria[19], were better using a lateral approach than anterior or posterior approach with 11% of patients undergoing fixation through a variety of lateral approaches obtaining a poor or bad result compared with 35% and 51%, respectively .
Some studies with the same technique used the Thompson-Epstein score for the reduction. Unfortunately, these Radiographic criteria of this classification are not based on the reduction performance but mostly on the arthritic features of the hip. We achieved an anatomic reduction in 14 patients according to Matta criteria. Furthermore, these studies did not specifically mention associated traumatic osteochondral lesions. In our study we found those injuries in three hips, which were not detectable on standard radiographs. This may explain the lack of correlation between unsatisfying intraoperative findings and apparently excellent reductions noted on early radiographs. The amount of residual fracture displacement may not correlate with clinical outcomes, although every effort should be made to obtain the best possible reduction [20-24].
Complications include AVN, progression to arthritis, and heterotopic ossification. The rate of AVN is our series was 5.6% and this is consistent with the reported literature. Giannoudis et al. calculated an AVN rate of 11.8% (48 of 405) at a mean follow up of 59.7 months. Although our rate is lower, our follow up was shorter.
In this study, at final follow up, Tönnis classification was found as Grade I in four patients, Grade III in one patient who underwent arthroplasty, but all remaining patients were classified as Grade 0. In this series superficial infection occurred in two patients treated conservatively using dressing and I V antibiotics.
Heterotopic ossification (including all Brooker grades) rate was 16.8% (68 of 405), but with the numbers available, no difference could be seen between surgical approaches . Our results recorded the heterotopic ossification rate was 16.2% of grade I. In this study, the lateral and posterolateral approaches with trochanteric flip osteotomy allowed 360° exposure and repair of lesions. This approach was used in a variety of nontraumatic hip pathologies and for selected types of acetabular fractures [22].
5. Conclusion
This technique is recommend for surgeons treating fracture femoral head with or without acetabular fractures as it provide full exposure of the femoral head. As a limitation of this study, the small number of cases and lake of previous study using the same technique for the same indication. Future studies are required to compare this approach with others regarding the outcome scores and complications.
References
- Droll KP, Broekhuyse H, O’Brien P. Fracture of the femoral head. J Am Acad Orthop Surg. 2007; 15(12):716–27.
- Henle P, Kloen P, Siebenrock KA. Femoral head injuries: which treatment strategy can be recommended? Injury. 2007; 38(4):478–88.
- Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83:1119–1124.
- Gardner MJ, Suk M, Pearle A, Buly RL, Helfet DL, Lorich DG. Surgical dislocation of the hip for fractures of the femoral head. J Orthop Trauma. 2005; 19:334–342.
- Giannoudis PV, Kontakis G, Christoforakis Z, Akula M, Tosounidis T, Koutras C. Management, complications and clinical results of femoral head fractures. Injury. 2009; 40:1245–1251.
- Gillespie P, Aprato A, Bircher M. Hip dislocation and femoral head fractures. In: Bentley G, editor. European Surgical Orthopedics and Traumatology: the Efort Textbook. Berlin, Heidelberg, Germany: Springer; 2014. pp. 2179–2202.Laorr A, Greenspan A, Anderson MW, Moehring HD, McKinley T. Traumatic hip dislocation: early MRI findings. Skeletal Radiol. 1995; 24:239– 245.
- Pipkin G. Treatment of Grade IV fracture-dislocation of the hip. A review. J Bone Joint Surg Am. 1957; 39:1027–1197.
- Alessandro M, Alessandro A, Caterina A, Marco F, and Reinhold G. Surgical Hip Dislocation Is a Reliable Approach for Treatment of Femoral Head Fractures. Clin Orthop Relat Res. 2015 Dec; 473(12): 3744– 3751.
- Massè A, Aprato A, Grappiolo G, Turchetto L, Campacci A, Ganz R. Surgical hip dislocation for anatomic reorientation of slipped capital femoral epiphysis: preliminary results. Hip Int. 2012; 22:137–144.
- Massè A, Aprato A, Rollero L, Bersano A, Ganz R. Surgical dislocation technique for the treatment of acetabular fractures. Clin Orthop Relat Res. 2013; 471:4056–4064. doi: 10.1007/s11999-013-3228-8.
- Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am. 1996; 78:1632–1645.
- Brooker A, Bowerman J, Robinson R, Riley LH. Ectopic ossification following total hip replacement: incidence and a method of classification. J Bone Joint Surg Am. 1955; 55:1629–1632.
- Tönnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976; 119:39–47.
- Ovre S, Sandvik L, Madsen JE, Roise O. Modification of the Harris hip score in acetabular fracture treatment. Injury. 2007; 38:344–349.
- Brooks RA, Ribbans WJ. Diagnosis and imaging studies of traumatic hip dislocations in the adult. Clin Orthop Relat Res. 2000; 377:15– 23.
- Henle P, Kloen P, Siebenrock KA. Femoral head injuries: which treatment strategy can be recommended? Injury Int J Care Injured. 2007; 38:478–488.
- Alonso JE, Volgas DA, Giordano V, Stannard JP. A review of the treatment of hip dislocations associated with acetabular frac tures. Clin Orthop Relat Res. 2000; 377:32–43.
- Solberg BD, Moon CN, Franco DP. Use of a trochanteric flip osteotomy improves outcomes in Pipkin IV fractures. Clin Orthop Relat Res. 2009; 467:929–933.
- Thompson VP, Epstein HC. Traumatic dislocation of the hip; a survey of two hundred and four cases covering a period of twenty-one years. J Bone Joint Surg Am. 1951; 33:746– 748.
- Collinge C, Archdeacon M, Sagi HC. Quality of radiographic reduction and perioperative complications for transverse acetabular fractures treated by the Kocher-Langenbeck approach: prone versus lateral position. J Orthop Trauma. 2011; 25:538–542.
- Mostafa MF, El-Adl W, El-Sayed MA. Operative treatment of displaced Pipkin type I and II femoral head fractures. Arch Orthop Trauma Surg. 2014; 134:637–644.
- Siebenrock KA, Gautier E, Woo AK, Ganz R. Surgical dislocation of the femoral head for joint débridement and accurate reduction of fractures of the acetabulum. J Orthop Trauma. 2002; 16:543–552.
- Sink EL, Beaulé PE, Sucato D, Kim YJ, Millis MB, Dayton M, Trousdale RT, Sierra RJ, Zaltz I, Schoenecker P, Monreal A, Clohisy J. Multicentre study of complications following surgical dislocation of the hip. J Bone Joint Surg Am. 2011; 93:1132–1136.
- Wamper KE, Sierevelt IN, Poolman RW, Bhandari M, Haverkamp D. The Harris hip score: do ceiling effects limit its usefulness in orthopedics? Acta Orthop. 2010; 81:703–707. doi: 10.3109/17453674.2010.537808.