


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Cerebral Venous Sinus Thrombosis, a Diagnostic Challenge to
Emergency Ophthalmic Practice
Dr. Sandhya.Ramachandra1*, Dr. Reshma Ravindra2, Dr. Apurva Shivaji Navale3
2.Senior Registrar, Department of Ophthalmology, Sri DevRaj Urs Medical College, Kolar.
3.Resident (DOMS), Department of Ophthalmology, Sri DevRaj Urs Medical College,Kolar.
Copyright : © 2019 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Evaluation of head ache remains challenging to an Ophthalmologist due to its myriad etiology and severity. Here is one such case where fundus examination at initial presentation could have probably helped in early diagnosis.
The purpose of this case report is to impress upon the fact that this potentially serious neurological disease may present to the ophthalmologist and a high index of suspicion can help in detecting early papilloedema, a common feature of cerebral venous sinus thrombosis. Prompt treatment including anti coagulant therapy and reduction of intra cranial pressure may help in averting serious neurological complications.
Cerebral venous sinus thrombosis, Papilloedema, Head ache, Abducent palsy
BD – Bis In Die
BP- Blood Pressure
CNS – Central Nervous System
CSF – Cerebrospinal Fluid
CVT – Cerebral Vein Thrombosis
ICP - Intra Cranial Pressure
Inj - injection
Mg – Milligram
Ml - Milliliter
MRI - Magnetic Resonance Imaging
Tab – Tablet.
1. Introduction
Evaluation of head ache remains challenging to an Ophthalmologist due to its myriad etiology and severity. Here is one such case where fundus examination at initial presentation could have probably helped in early diagnosis.
2. Case Report
A 42 year old female presented with intolerable & distressing headache of 2 days duration. It was continuous, throbbing, in the temple and back of the head. The headache was present since 6 months, increased in severity since 20 days. Earlier it was intermittent, mild and relieved with rest. There was no history of trauma, fever, vomiting, seizures, and visual disturbances. She was not on treatment for any other ailment. There was no history of use of oral contraceptives. She gave history of loss of appetite, irregular menstrual cycles with scanty flow since 1 year. Family history was non contributory, she has 2 children aged 21 & 16 with normal pregnancy followed normal delivery, both times. There was no history of oral contraceptive usage.
The patient had consulted a physician who had treated with analgesics. Due to the persistence of headache, a neurologist was consulted & MRI was obtained. The MRI was normal as per the patient’s history. MRI was not available for our review. The patient was diagnosed and treated for migraine. The headache was not relieved with analgesics & anti migraine treatment.
The patient presented to our emergency medicine department with complaints of vomiting, 5 – 6 episodes, weakness and occasional involuntary movements of the right upper & lower limb. She complained of 2 episodes of urinary incontinence and disturbed sleep. She also gave history of chronic headache the character of which had changed with radiation to the neck. She complained of inability to open her eyes in the normal daylight. The patient was then admitted in the Medical Intensive Care Unit for which she was treated and was then referred to ophthalmology for an emergency fundus examination.
General physical examination showed a moderately built and nourished female, conscious, oriented & co- operative. She had severe photophobia, was irritable. She was afebrile, pulse 86beats / minute, regular, BP 150/90 mm Hg, mild pallor was present. Respiratory system, Cardio vascular system, per abdominal examination were normal with no organomegaly. CNS examination was essentially normal. The patient was referred for emergency ophthalmic opinion.
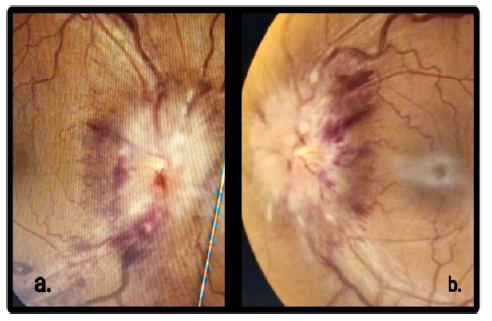
Ophthalmic evaluation was done - Both eyes showed normal adnexa and anterior segment, pupil was 2 mm in both eyes with well sustained reaction (severe photophobia was present), distant visual acuity was 6/ 6, near N8 in both eyes, colour vision was normal, intra ocular pressure was 12 mm Hg, extra ocular movements were full & normal , slit lamp examination of anterior segment was normal, media was clear, ophthalmoscopic examination revealed hyperaemic disc with blurring of the nasal margins, the cup was discernible, with cup disc ratio was 0.3, arterio - venous ratio was 2:4 with dilated tortuous veins at the posterior pole, there were no spontaneous or induced venous pulsations, foveal reflex was present , vessels & background retina was normal. Diagnosis of Early Papilloedema was made.
Investigations showed normal Erythrocytic Sedimentation Rate, peripheral smear showed normocytic, normochromic anaemia with leucocytosis. Serum electrolytes, liver function tests & renal function tests were normal. Fasting glucose, serum homocysteine, serum folic acid, vitamin B 12 levels were normal, anti nuclear antibodies & anti phospholipid antibodies were negative. Routine urine test was normal. Chest X- ray was normal, tuberculosis was ruled out.
Follow up examination after 72 hours, showed similar anterior segment findings with total obliteration of the cup, increased disc edema extending circumferentially with peripapillary hemorrhages and increased vascular tortuosity. Fovea was normal in both eyes.
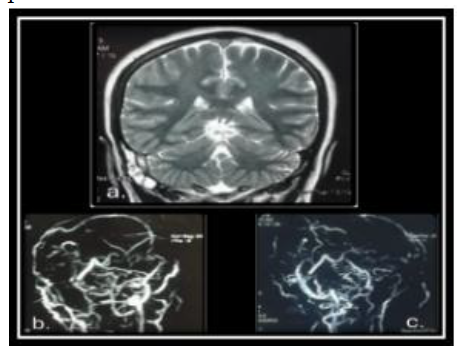
MRI brain was done, which showed T1 hyper intense, T2 heterogenously hyper intense signals were seen in posterior 2/3 rds of superior sagittal, transverse & sigmoid sinuses and in the cortical veins draining to superior sagittal sinuses & visualized segments of right internal jugular vein. Cerebral hemispheres showed late subacute intraparenchymal hematoma in the right temporal lobe with subarachnoid haemorrhages in the bilateral perirolandic regions and right temporal lobe cortical sulci. Thalami, basal ganglia, cerebellum, pons, medulla were normal. Mild cerebral oedema and papilloedema was seen. Partially empty sella was seen & there was bilateral prominent peri neural sheaths of intra orbital segments of optic nerve with mild tortuosity. Mild & diffuse thickening of pachymeninges was present, no midline shift or mass effect was seen. Mucosal thickening of bilateral ethmoid sinuses, left frontal sinus & fluid signal in the right mastoid air cells suggestive of chronic paranasal sinusitis was noted. Lumbar puncture & CSF analysis were not done in view of the venous sinus thrombosis and parenchymatous brain lesions, partial empty sella & enlarged perioptic spaces.
The patient was diagnosed with cerebral venous sinus thrombosis. She was started on Tab. Nicoumalone 2mg OD, Tab. Levetiracetam 500mg BD, Inj. Piperacillin with Tazobactam 4.5mg TID, Inj Tramadol 1 ampule SOS and Tab. Tramadol BD. Inj. Mannitol 100ml BD, was started as an anti edema measure.
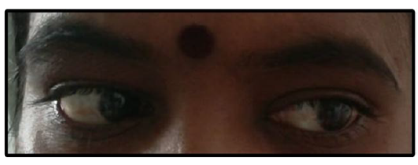
After 1 week of initial presentation, the patient was referred back as she complained of diplopia. On examination, the patient had left lateral rectus paresis – Abducent nerve paresis, with? ill sustained right pupillary reaction, other anterior segments findings were the same as before. Fundus showed full blown papilloedema, superficial nerve fibre hemorrhages in the peripapillary area and few exudates were seen in the macular area of left eye. The disc elevation was more that 4 Diopters in both eyes. On the following day, the left Aducent paresis had worsened with diplopia in primary gaze. Thereafter, there was no symptomatic worsening of diplopia.
Same treatment was continued and the antibiotic course was completed. Mannitol 100ml BD was given for 5days. At discharge, the patient was symptomatically better. The head ache, vomiting & diplopia in primary gaze had resolved. Bilateral papilloedema was present, visual acuity was maintained at 6/6 & N6. All drugs except anti coagulants were stopped.
3. Discussion
Papilloedema is an important ophthalmoscopic sign due to multiple etiologies. The term “papilloedema” indicates swelling of the optic discs secondary to increased intracranial pressure. Intra cranial space occupying lesions, head injuries, cerebral hemorrhage and impaired cortical or cerebral sinus venous drainage are some of the known causes. Idiopathic intra cranial hypertension is essentially a diagnosis of exclusion. Various mechanisms have been proposed to describe the pathogenesis of the papilledema in intracranial hypertension. Increased pressure around optic nerve causes axoplasmic flow stasis in the prelaminar nerve fibers and also there is venous congestion due to compression of draining veins which are also compressed by axonal swelling, interstitial edema resulting in disc edema. The vascular changes seen clinically are secondary & may not have a causative role [1].
Cerebral venous sinus thrombosis is a cerebrovascular event among the younger age groups, with diverse clinical presentation. The incidence of CVT may be 1.32-1.57 per 1,00,00 person years [2], requiring greater attention as the prognosis may be poor in some patients.
The patient presented with acute neurological symptoms, including weakness of limbs suggesting onset of stroke. Stroke in the young, although uncommon, may be caused by cortical & dural venous sinus thrombosis [3].
The patient gave a history of change in the character & intensity of headache, weakness of limbs, incontinence & vomiting and irritability of recent origin. It is imperative to remember in emergency room evaluation that, cerebral venous thrombosis often presents with headache, with variable neurological signs & symptoms [4]. As in this patient, a history of recent change of character of chronic head ache is to be specifically asked for.
In CVT, headache, elevated intra cranial pressure, papilloedema are mainly because of the superior sagittal sinus involvement [5] 89% of patients with cerebral venous & dural sinus thrombosis (CVT) present with headache as their initial symptom. The venous outflow impediment through the large sinuses is the cause of intra cranial hypertension, papilloedema & headache [6]. The venous outflow obstruction resulting in elevated CSF pressure is the main cause of all clinical symptoms in CVT [7].
The diagnosis remains a challenge due to the diverse etiology, associated risk factors and absence of standard treatment protocols. Cortical & dural venous sinus thrombosis is diagnosed clinically based on a high index of suspicion and confirmed by imaging. The clinical features are attributed to the raised intracranial pressure or to the focal brain injury as a result of venous ischaemia, infarction or hemorrhage. Both mechanisms may contribute to the clinical spectrum at presentation or during the course of the disease as seen in this case [8].
International Study on Cerebral Vein & Dural Sinus Thrombosis (ISCVT) revealed that papilloedema is a common clinical feature & it may be present in about 28% of the patients [9].
The Abducent palsy that occurred during the course of evolution of papilloedema is the most common false localizing sign, typically seen in elevated intra cranial pressure. It may be unilateral or bilateral. It is attributed to the stretching of the nerve in its long intracranial course or compression against the petrous ridge or petro clinoid ligament [10].
In this patient, the Abducent palsy evolved during the course of hospital stay and worsened causing disturbing diplopia to the patient, then stabilized with recovery of abduction after 72 hours, suggesting good response to ongoing treatment. There was no worsening of neurological deficits, including stoke which is potentially debilitating.
Papilloedema, by definition is invariably associated with elevated intracranial pressure but elevated intra cranial pressure (ICP) can exist without papilloedema. Presence of spontaneous venous pulsations suggests that ICP may not be very high at that time. In this patient we documented rapid progression of papilloedema and Abducent palsy during the course of treatment. Headache, specific or vague neurological symptoms in young adult women must have differential diagnosis of CVT, a potentially fatal entity with mortality of over 30%, as reported in literature. Prompt diagnosis with modern imaging techniques has helped in early treatment and better prognosis.
4. Conclusion
The purpose of this case report is to impress upon the fact that this potentially serious neurological disease may present to the ophthalmologist and a high index of suspicion can help in detecting early papilloedema, a common feature of CVT. Prompt treatment including anticoagulant therapy and reduction of intra cranial pressure may help in averting serious neurological complications.
The drawbacks of the study was that other pro thrombotic factors like – anti phospholopid antibodies, antithrombin III, protein C, protein S, factor V Leidedn positivity, etc. are yet to be evaluated. Behcet’s syndrome & SLE also need to be ruled out [11].
5.References
- Hayreh SS.Pathogenesis of optic disc edema in raised intracranial pressure.Progress in retinal and eye research.2016 Jan; 50: 108-44.
- Luo Y, Tian X, Wang X. Diagnosis and Treatment of Cerebral Venous Thrombosis: A Review. Frontiers in aging neuroscience. 2018 Jan; 10: 2.
- Bousser MG, Ferro JM. Cerebral Venous thrombosis: an update. The Lancet Neurology. 2007 Feb; 6 (2): 162-70.
- Kimber J. Cerebral venous sinus thrombosis. QJ Med 2002; 95: 137 – 42.
- Biousse V, Ameri A, Bousser MG.Isolated intracranial hypertension as the only sign of cerebral venous thrombosis. Neurology. 1999 Oct; 53 (7): 1537.
- Coutinho JM, Gerritsma JJ, Zuurbier SM, Stam J. Isolated cortical vein thrombosis: systematic review of case reports and case series. Stroke. 2014 Jun; 45 (6): 1836 -8.
- Bansal BC, Gupta RR, Prakash C. Stroke during pregnancy and puerperium in young females below the age of 40 years as a result of cerebral venous / venous sinus thrombosis. Japanese heart journal. 1980; 21 (2): 171-83.
- Saponski G, Barinagarrementeria F, Brown RD, Bushell CD, Cucchiara B, Ferro JM, Et Al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/ American Stroke Association Stroke.2011 Jan;42: 1158 – 1192.
- Ferro JM, Canhao P, Stam J, Bousser MG, Barinagarrementeria F. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004 Mar; 35 (3): 664-70.
- Collier J. The false localizing signs of intracranial tumour. Brain. 1904 Jan; 27(4): 490-508.
- Daif A, Awada A, Al- Rajeh S, Abdulijabbar M, Al Tahan AR, Obeid T, et Al. Cerebral venous thrombosis in adults: a study of 40 cases from Saudi Arabia. Stroke. 1995 Jul; 26(7): 1193 -5.