


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Child with Penetrating Orbital Injury as a Result of Assault
Lawan Abdu1*, Usman Abubakar Mijinyawa2
2.Department of Ophthalmology, Murtala Muhammad Specialist Hospital, Kano -Nigeria.
Copyright : © 2018 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: A 3 year old child was assaulted by an adult with a stick that broke and a piece of it stuck in the patient’s left orbit.
Case description: The patient was referred from another hospital after the parents noticed the wood jutting out of the left orbit with associated pain, swelling and discharge. There was associated loss of vision. However there was no history of fever or loss of consciousness.
Clinical findings: There was left eye discharge with a piece of the wood that had bruised the cornea. The patient could recognize common objects after gentle parting of the lids. He was reviewed by the neurosurgeons to rule out intra cranial involvement. Cranial CT scan showed the foreign body was limited to the orbit with no intra ocular involvement. The patient was placed on broad spectrum intra venous antibiotic cover, anti tetanus sera was administered as well as analgesics. After routine preliminaries and under general anesthesia the object was lifted off the eye followed by careful dissection; manipulation and extraction form the orbit. The post operative condition was monitored till satisfactory recovery was achieved.
Conclusion: A case of assault resulting in penetrating orbital injury with foreign bod y retention is reported. There was no associated intra ocular and intra cranial injuries and recovery was satisfactory with appropriate surgical intervention.
Assault, Orbit, Injury, Foreign body, Infection, Surgery ,Ophthalmology
1. Introduction
Penetrating orbital injuries occur infrequently in civil life. Such injuries maybe globe sparing and affect orbital structures only. There are reports indicating penetrating orbital injuries can be sight and even life threatening[1]. Severe brain injury was observed in association with trans-orbital intracranial injury. Though quite rare occurring in 0.04%, it can lead to severe brain damage and even death[2]. Penetrating orbital injuries in children are usually accidental in most cases, but sometimes it could be as a result of an assault. This report provides the management of a 3-year old boy who had orbital injury caused by a piece of wood which penetrated through the inter-palpebral fissure into the left orbit.
2. The Case
A 3 year old Fulani child from Daura in north western Nigeria was referred from a general hospital with the history of foreign body in the left eye. The informant was the father who claimed patient was assaulted by an adult with a wooden stick 3 days prior to presentation and a piece of wood broke and hit the patient in the left orbit. The patient was said to have fallen on the face driving the wooden piece deeper. There was pain and bleeding from the site. The patient was able to see with the said eye. There was no history of loss of consciousness, convulsion, vomiting or fever during the period. Patient was taken to two different hospitals before he was referred to our centre. He was placed on unspecified parenteral medications. There was no formal referral document. On examination, the patient was afebrile, not pale and well oriented in time place and person. The Right eye was essentially normal. Patient could recognize common objects presented with the injured left eye after gentle parting of the palpebral fissure.
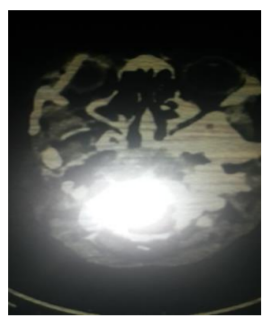
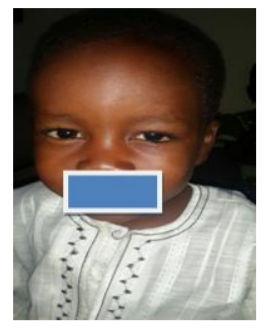
There was purulent discharge in left eye and the lid was swollen and tender. A piece of hard, fixed wood [Figure 1] was observed passing in the inter-palpebral fissure lateral to the globe, displacing and hindering visualization of the globe. Patient was reviewed by Neurosurgeons. The general condition of the patient was stable and there were no clinical signs of neurological deficits. Investigations done includes; hemoglobin level, random blood sugar, urea and electrolytes which were all within normal limits. A head CT scan was done to identify the position of the foreign body (FB) and its relation to surrounding structures. The FB (Figure 2) was entirely intra orbital (Figure 3). The anesthesiologist reviewed and certified patient fit for general anesthesia.


3. Preliminary Treatment
Patient had a dose of anti-tetanus serum (1500 iu), and was placed on intra venous clavulanate potentiated amoxicillin, metronidazole, paracetamol and appropriately determined volume of pediatric saline fluid. Informed consent was administered and patient was prepared for exploration and removal of foreign body.
4. Procedure
After routine cleaning and draping, lids were parted open with a speculum. Blunt dissection of the conjunctiva was performed at the edges of the wood; the piece of wood was carefully lifted off the cornea, manipulated and removed. There was slight lower lid abrasion and moderate conjunctiva chemosis. The globe was visualized and was intact despite inferior corneal abrasion caused by direct contact with the piece of wood. The wound site was further explored and irrigated with saline to remove any residual fragments. The potential space was filled up with chloramphenicol eye ointment, and the outer edges of the wound sutured with 6/0 vicryl. Subconjunctival dexamethasone 4mg and gentamicin 20mg was given. An eye pad was applied and tapped with tissue plaster. Patient was maintained on systemic antibiotics. Topical antibiotic steroid combination eye drop was administered hourly for the first 24 hours then four times a day.
The patient was discharged after five days with improvement in vision. Figures 4, 5 and 6 showed the eye of the patient at 1, 2 and 14 days after surgery. There was remarkable recovery within two weeks. The left eye was normal except for small nebula opacity near the limbus between 5 and 6 o’clock position.


5. Discussion
Orbital trauma could be penetrative or blunt. Penetrating injury could be through the skin and bone into the orbit, through the lid and sometimes even through the inter palpebral fissure. Different types of materials can penetrate into the orbit such as arrow injury,3 glass, wooden objects, and metals[2]. Sharp edge wooden foreign body penetrating deep into the orbit can even extend into the cranial cavity. Globe is at risk of damage from penetrative injury. However, a study had shown that some patients had penetrating injury to the orbit without any damage to the globe[2]. Orbital injury from penetrating object is determined by the location of the wound entry, speed, and shape of the penetrating object, as well as physical characteristics of the intra orbital contents[4]. In Zaria, penetrating orbital/ocular injury accounted for 4.2% of trauma cases[5]. Wooden intra-orbital foreign body can be of various forms as shown in a study that reported pencil accounting for 39% of cases, tree branch/ plant matter (35%), and other treated wood in 26% of cases[4]. In these case report we found a piece of sharp edge wooden object, that penetrated through some of the orbital spaces/orbital fat passing the peripheral, central and even the sub periosteum close to the got ethmoid bone.
The associated infection was not too florid although a study indicated that orbital cellulitis could occur as a complication of such injuries[7]. there was globe perforation and vision was restored. There has to be mechanism to protect vulnerable groups particularly children from all forms of assaults that could lead to pain and disability.
References
- Cleary G, Nischal KK, Jones CA. Penetrating orbital trauma by stiletto causing complex cranial neuropathies . Emerg Med J. 2006 Apr; 23(4): e28. doi: 10.1136/emj.2005.029983
- Mehmet A, Metehan E, Burhan OG, Ismail D. Trans-orbital orbito-cranial penetrating injury caused by a metal bar. J Neurosci Rural Pract. 2012 May-Aug; 3(2): 178–181.doi: 10.4103/ 0976-3147.98228
- Lawan A, Danjuma SA. Arrow injury to the eye. Ann Afr Med 2012; 11:116-118.
- Jerome RH, Russell WN, Henry IB. Penetrating orbital trauma. Am J Emerg Med 1983; 1(1): 22-27.
- Rafindadi AL, Pam VA, Chinda D, Mahmud AF. Orbital and ocular trauma at Ahmadu Bello University Teaching Hospital, Shika–Zaria; A retrospective review, Ann Nig Med 2013;7: 20 23.
- Shelsta HN, Bilyk JR, Peter AD, Penne RB, Carrasco JR. Wooden intra-orbital foreign body injury; clinical characteristics and outcomes of 23 patients. Ophthalmol Plast Reconstr Surg 2010; 26 (4):238-244.
- Balogun BG, Balogun MM, Adekoya BJ. Orbital cellulitis: clinical course and management challenges. The Lagos State University Teaching Hospital experience Nig Q J Hosp Med. 2012 Oct-Dec; 22(4):231-5.