


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Bilateral Simultaneous Non-Arteritic Anterior Ischemic Optic Neuropathy in Association with Alcoholic Fatty Liver Disease: A Case Report
Dr. Sohraab Yadav*1, Ms. Alison Rowlands1
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
We present a unique case of bilateral simultaneous non -arteritic anterior ischemic optic neuropathy (NAION) in association with alcoholic fatty liver disease in a 68 year old male. The patient presented with acute visual field loss and jaundice. The history revealed increased short -term alcohol intake. Eye examination, visual field testing and imaging were consistent with anterior ischemic optic neuropathy. Inflammatory markers were normal and there were no vascular risk factors. Liver function tests were acutely deranged and further investigations showed only fatty ch anges. Here we highlight the importance of alcohol intake enquiry in NAION patients, particularly those presenting with bilateral disease.
non-arteritic, ischemic optic neuropathy, simultaneous, alcohol, fatty liver1. INTRODUCTION
Bilateral simultaneous non-arteritic anterior ischemic optic neuropathy (NAION) is exceptionally rare and is usually found in association with severe hypotension resulting from blood loss [1, 2].
2. CAS E REPORT
A 68 year old male retired engineer presented to the eye clinic with a sudden onset inferior visual field defect in both eyes since waking. There were no associated headaches or jaw claudication. The patient had been feeling more lethargic over the past 10 weeks, had been passing dark urine and appeared to be slightly jaundiced in appearance. There was no history of vascular risk-factors such as diabetes or hypertension.
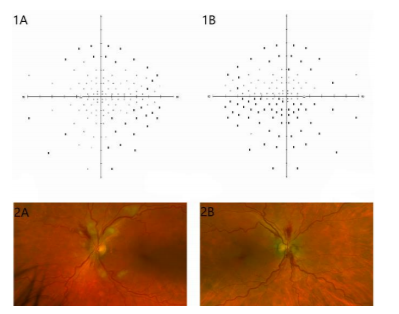
Distance visual acuity was 6/6 in the both eyes. Color vision testing was not possible due to a history of red/green colour-blindness. Temporal artery pulsation was strong and equal on both sides. Formal visual field testing revealed bilateral dense inferior and moderate superior field defects (figure 1 A and B). Dilated fundal examination revealed bilateral optic disc swelling and splinter haemorrhages (figure 1 C and D).
Blood tests showed normal full blood count, ESR, CRP and coagulation profile. Given the clinical features, liver function tests were ordered. These were grossly deranged with bilirubin measuring 81 micromol/l, ALP 278 IU/L, AST 140 IU/L, ALT 64 IU/L and GGT 2903 IU/L. The results prompted an inpatient admission under the medical team. Further questioning revealed the patient had been drinking approximately 16 units of alcohol every day for the past year. Medical examination did not identify features of chronic liver disease. Investigations included a negative HIV antibody/p24 test, negative CMV IgM, negative Coxsackie virus PCR and negative Hepatitis A/C/E IgM. The Hepatitis B antibody profile conferred immunity. Nutritional deficiencies were excluded and serum homocysteine was normal. Ultrasound scanning of the liver showed fatty liver changes with no focal lesions or biliary abnormalities. A full body CT, liver MRI and magnetic resonance cholangiopancreatography showed only fatty nodular deposition in the liver with no evidence of malignancy. Carotid Doppler failed to identify a significant stenosis of either internal carotid artery.
The patient was ultimately given a diagnosis of alcoholic fatty liver disease with acute liver decompensation. On latest follow-up the patient’s liver profile has improved but he has developed a right relative afferent pupillary defect and bilateral optic nerve pallor. The progression of his signs and symptoms, optical coherence tomography and visual fields were consistent with a diagnosis of bilateral simultaneous NAION. Formal electro diagnostic testing identified a reduction of visual evoked potentials (VEP) from both eyes but no significant delay. Final central visual acuity remained 6/6 in both eyes.
3. DISCUSSION
NAION is thought to be multifactorial in origin. Typically the optic disc has a distinct small and crowded anatomy. Patients usually have vascular risk factors such as diabetes, hypertension and hyperlipidemia. No effective treatment exists although there is some evidence for the benefit of steroid treatment for these cases [3]. Most Bilateral simultaneous NAION is exceptionally rare and is usually found in association with severe hypotension resulting from blood loss and acute compromise to the optic nerve circulation [1, 2].
The main differential that required exclusion in our patient was bilateral optic neuritis. Color-vision testing was not possible in our patient but the history of painless reduction in visual field, no pain on eye movements and no delay in VEPs was consistent with NAION.
Bilateral simultaneous NAION has not previously been reported in association with fatty liver disease and short term increased alcohol intake which were the only identifiable risk factors in our patient. There have been other documented associations between liver disease and the development of this condition. It may be seen as an extra hepatic manifestation of active viral and auto-immune hepatitis and its treatment which were ruled out on serological testing for our patient [4]. Longstanding alcoholic liver cirrhosis has been reported as a cause but our patient lacked these clinical features and did not have a long history of excessive alcohol intake [5].
There is limited evidence on the mechanism of NAION in liver disease. Despite the well-recognised bleeding tendency due to lack of coagulation products in end-stage liver disease, patients with liver dysfunction may develop a temporary hypercoagulable state due to haemodynamic and secreted factor imbalances [6]. This may lead to acute ischemia of the optic nerves similar to the event that occurred in our patient. Given the association, alcohol intake enquiry in NAION patients is important. Further research is needed on the role of anticoagulation or other preventative treatment in at-risk liver disease patients.
References
- Giusti, C., Bilateral non-arteritic anterior ischemic optic neuropathy (NA -AION): case report and review of the literature. Eur Rev Med Pharmacol Sci, 2010. 14(2): p. 141-4.
- Yazgan, S., et al., Simultaneous Bilateral Non - Arteritic Anterior Ischaemic Optic Neuropathy and Unilateral Central Retinal Artery Occlusion after Hip Prosthesis Surgery. Neuroophthalmology, 2014. 38(5): p. 257-259.
- Hayreh, S.S. and M.B. Zimmerman, Non - arteritic anterior ischemic optic neuropathy: role of systemic corticosteroid therapy. Graefes Arch Clin Exp Ophthalmol, 2008. 246(7): p. 1029-46.
- Prud'homme, S., F. Nevens, and I. Casteels, Bilateral simultaneous anterior ischemic optic neuropathy, an extrahepatic manifestation of hepatitis C cured with direct acting antivirals. GMS Ophthalmol Cases, 2016. 6: p. Doc05.
- Bassi, S.T. and A. Dasgupta, Bilateral simultaneous nonarteritic anterior ischemic optic neuropathy in a patient with alcoholic liver disease. Oman J Ophthalmol, 2014. 7(2): p. 72-4.
- Stine, J.G. and P.G. Northup, Coagulopathy Before and After Liver Transplantation: From the Hepatic to the Systemic Circulatory Systems. Clin Liver Dis, 2017. 21(2): p. 253-274.