


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
ARC Journal of Ophthalmology
Volume-1 Issue-1, 2016, Page No: 19-22
Spontaneous Resolution of Vitreomacular Traction in a Patient with a Macular Hole in the Fellow Eye
Leopoldo Spadea, MD1, Francesca Verboschi, MD1, Carlo Cagini, MD2, Salvatore Cillino, MD3
1 Department of Biotechnology and Medical-Surgical Sciences, “Sapienza” University of Rome, Latina, Italy
2 Department of Surgical and Biomedical Sciences, University of Perugia, Perugia, Italy
3 Eye Clinic, Policlinico P. Giaccone, University of Palermo, Palermo, Italy.
2 Department of Surgical and Biomedical Sciences, University of Perugia, Perugia, Italy
3 Eye Clinic, Policlinico P. Giaccone, University of Palermo, Palermo, Italy.
Citation : Leopoldo S, Francesca V, Cagini C, Cillino S. Spontaneous Resolution of Vitreomacular Traction in a Patient with a Macular Hole in the Fellow Eye. ARC Journal of Ophthalmology. 2016;1(1):19–22.
Copyright : © 2016 Leopoldo S. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Vitreomacular traction (VMT) is a multicategory entity that may cause substantial visual loss due to the formation of a macular hole or traction-induced tissue distortion. We report a remarkable case of spontaneous resolution of VMT in a 76-year-old caucasian female who presented a reduction visual acuity in one eye and a macular hole stage IV with margins edema in the other eye. The patient denied any treatment and was followed over time with optical coherence tomography (OCT) which showed the evolution of the vitreomacular adhesion and then the subsequent spontaneous detachment with a complete visual acuity recovery. Therefore the therapeutic decision must be guided from the evaluation of the visual acuity, fundus appearance and OCT performed over time.
This case report demonstrates how the same macular traction has led to two different outcomes in the two eyes at different times and ways; not always the course of an eye is the same in the other eye.
Keywords: Vitreomacular Traction, Pars Plana Vitrectomy, Ocriplasmin, Optical Coherence Tomography.
1.Introduction
Vitreomacular traction (VMT) syndrome was described for the first time in 1967 as partial peripheral detachment of the vitreous with preserved posterior attachment to the macula [1]. In observational and interventional studies, the mean age of patients is around 65–75 years, with a predominance of females [2]. If the traction appears within the peripheral retina, it causes a regmatogenous retinal detachment. If it appears within the macula, it causes a VMT syndrome or a macular hole. The course of the disease is largely determined by the traction placement (focal or wide-based) and by the degree of posterior vitreous detachment (PVD) [3]. We report the case of a patient with bilateral VMT resolved spontaneously in one eye and evolved in macular hole in the contralateral eye.
2. Case Presentation
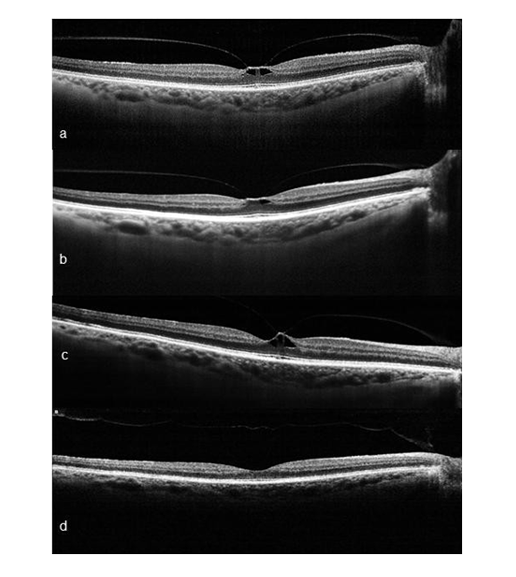
A caucasian female aged 76 years presented in December 2010 for a reduction of visual acuity in left eye (LE). In anamnesis the patient reported only an hypercholesterolemia in drug therapy; she denied history of eye disease. The distance corrected visual acuity (DCVA) was 20/20 in right eye (RE) and 20/200 in LE. The examination of the anterior segment in both eyes revealed a normal bulbar conjunctiva, transparent anterior chamber and a clear cornea; only an initial cortical cataract was evidenced. The fundus examination in RE revealed normal optic disc, trophic macula, mild angiosclerosis and normal periphery of retina; while in LE there was a macular hole stage IV with perilesional edema confirmed by optical coherence tomography (OCT, iVue, Optovue Inc., Fremont, CA, USA) (Figure. 1a). In April 2014, the patient reported a decreased visual acuity in RE with metamorphopsia, photopsia, and micropsia: visual acuity was 20/25 in RE and 20/200 in LE. The slitlamp examination and intraocular pressure were unremarkable in both eyes, fundus examination showed a vitreomacular traction in RE, while unchanged situation in LE. OCT in RE revealed an incomplete posterior vitreous detachment with broad vitreous adhesion at the macular area, which had resulted in thickening, distortion, edema of the fovea and adjacent retina, and foveal thickness increased to 298 μm (Figure. 2a). The maximal diameter of the adhesion was 918 μm in horizontal scans and 1153 μm in vertical scans. The patient was proposed treatment with a molecule like plasmin or pars plana vitrectomy but she refused any treatment. The patient was followed over time and November 2014 a worsening of visual acuity and ophthalmoscopy framework proven by OCT was observed (Figure. 2b). Foveal thickness increased to 332 μm owing to adhesion at the fovea, the maximal diameter of the adhesion increased to 930 in horizontal scans and to 1172 μm in vertical scans. In June 2015 the patient showed further deterioration: the visual acuity decreased to 20/40, and the OCT showed a foveal thickness increased to 378 μm, the maximal diameter of the adhesion was 951 μm in horizontal scans and 1270 μm in vertical scans (Figure. 2c).
In November 2015 the patient reported a spontaneous improvement in visual symptoms: the DCVA in RE was 20/20, and OCT revealed the reduction of foveal thickness (254 μm) and a complete posterior vitreous detachment without macular traction (Figure. 2d) while in LE persisted a macular hole stage IV (Figure. 1b).
Figure1. Macular hole stage IV in LE of the patient from the first diagnosis (December 2010) (A) to the last OCT after five years (b).
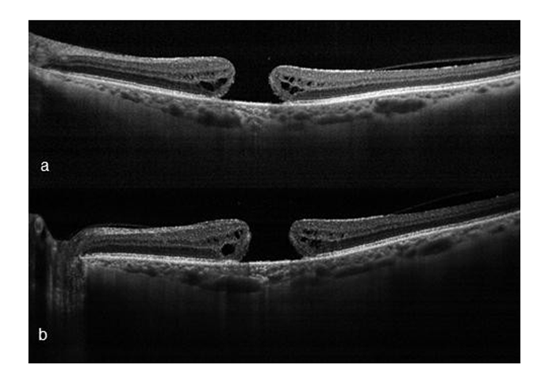
Figure2. First diagnosis of VMT in April 2014 (a); evolution after 15 days (b); worsening of the pattern and the symptoms in June 2015 (c); complete spontaneous resolution of VMT 19 months after the first diagnosis (d) in which there is a decrease in the VMT area and foveal thickness.
3. Discussion
Vitreomacular traction syndrome is characterized by anteroposterior traction on the macula, resulting from persistent vitreous adhesion at the macular area during incomplete PVD [4]. Symptoms such as decreased visual acuity, metamorphopsia, photopsia, and micropsia are common. Gass identified the VMT as a cause of macular hole first stage in the classification of macular holes [5]. VMT can be subclassified by the diameter of vitreous attachment to the macular surface as measured by OCT, with an attachment of 1500 μm or less defined as focal and an attachment of more than 1500 μm as broad. When associated with other macular disease, VMT is classified as concurrent. Full-thickness macular hole (FTMH) is a foveal lesion with interruption of all retinal layers and it is primary if caused by vitreous traction or secondary if directly the result of pathologic characteristics other than VMT. FTMH is subclassified by size of the hole as determined by OCT and the presence or absence of VMT [6].
The course of the disease is largely determined by the traction placement (focal or wide-based) and by the degree of PVD. Membrane traction within the fovea most often results in macular edema, and may even lead to the development of a macular hole.
Pars plana vitrectomy represents a definitive solution for VMT. In many cases, elimination of vitreoretinal traction and complete separation of the posterior hyaloid from the retinal surface with removal of all vitreous gel lead to both anatomic and functional improvement. Though outcomes have improved with advancements in instrumentation and technique, the utility of vitrectomy remains limited by incomplete vitreoretinal separation and vitreous removal, associated complications, and high costs [7].
There are also agents used for pharmacologic vitreolysis categorized as “enzymatic” or “nonenzymatic” according to their mechanism of action. The majority of proposed agents for pharmacologic vitreolysis are enzymes which include but are not limited to tissue plasminogen activator (tPA), plasmin, microplasmin, nattokinase, chondroitinase, dispase, and hyaluronidase. Among enzymatic agents there is plasmin [8]. Ocriplasmin is a recombinant human protein which contains plasmin’s catalytic domain [9], injected into the vitreous, it induces a PVD by cleaving the extracellular matrix that adheres the vitreous to the internal limiting membrane of the retina [10,11]. Ocriplasmin is more stable than autologous plasmin, has increased sterility, and is one-fourth the size of plasmin (22 kDa versus 88 kDa), which likely facilitates greater penetration of vitreous and epiretinal tissues [12]. The safety profile of ocriplasmin has been evaluated in a number of clinical studies. Adverse events included vitreous floaters, conjunctival hemorrhage, photopsia, and injection- related eye pain, secondary macular hole, retinal detachment and reduced visual acuity [13].
In a small number of cases, VMT resolves spontaneously without intervention (reported incidences are 10–11%) [14]. The tenacity of the adhesion between the vitreous gel and macula determines the likelihood of spontaneous PVD. There are currently no published consensus guidelines for the management of VMT. However, some general recommendations can be made. Patients should be observed for 2–3 months to see if spontaneous resolution occurs, although this is dependent on symptom severity and impact on the individual patient’s quality of life. If there is no resolution, treatment with ocriplasmin should be considered, taking into account factors such as the width of the VMT, presence of epiretinal membrane, the status of the affected eye’s lens, and patient age [13]. Surgery, as opposed to ocriplasmin is recommended if significative epiretinal membrane is present.
There are many factors affecting the prognosis of VMT. Odrobina et al.[15] reported a spontaneous resolution of VMT in up to 47% of eyes without epiretinal membrane and they concluded that vitreous surface adhesion and persistence of epiretinal membrane may be the prognostic factors for the natural course of VMT. Wang et al. demonstrated a case of spontaneous resolution in a patient without cystoid macular edema, epiretinal membrane or other maculopathy [16]. Yamada et al. [17] proposed two types of VMT to predict the postoperative outcome: the V-shaped pattern was a partial V-shaped PVD nasally and temporally, suggesting a favorable surgical outcome; the J-shaped pattern was a partial PVD temporal to the fovea in which prominent cystoid macular edema might develop and result in a macular hole or macular atrophy postoperatively. The eyes with VMT frequently had concurrent epiretinal membrane. Carpineto et al. also reported the case of a 34-year-old woman [18] with VMT and secondary CME. This patient also ended up with spontaneous resolution and complete restoration of her DCVA.
These studies, however, reported cases of unilateral VMT and subsequent resolution.
The peculiarity of the present study concerns the case of a single patient who had a different evolution of the same VMT in the two eyes: a spontaneous resolution of VMT with positive effects on visual acuity in one eye, while in the other eye VMT leads to the formation of a macular hole with severe visual impairment. Actually there are no guidelines to predict the trend of vitreomacular adhesion and to decide to undergo treatment. The therapeutic decision must be guided from visual acuity, fundus appearance and OCT performed over time.
References
- Jaffe N. S., Vitreous traction at the posterior pole of the fundus due to alterations in the vitreous posterior, Trans. Am. Acad. Ophthalmol. Otolaryngol. 71(4), 642–652 (1967).
- Jackson T.L., Nicod E., Simpson A., Angelis A., Grimaccia F. and Kanavos P., Symptomatic vitreomacular adhesion, Retina. 33(8), 1503–1511 (2013).
- Raczyńska D., Lipowski P., Zorena K., Skorek A. and Glasner P., Enzymatic vitreolysis with recombinant tissue plasminogen activator for vitreomacular traction, Drug Des. Devel. Ther. 27(9), 6259–6268 (2015).
- Bottós J.M., Elizalde J., Rodrigues E.B. and Maia M., Current concepts in vitreomacular traction syndrome, Curr. Opin. Ophthalmol. 23(3), 195-201 (2012).
- Gass J.D., Reappraisal of biomicroscopic classification of stages of development of a macular hole, Am. J. Ophthalmol. 119(6), 752–759 (1995).
- Duker J.S., Kaiser P.K., Binder S., de Smet M.D., Gaudric A., Reichel E., Sadda S.R., Sebag J., Spaide R.F. and Stalmans P., The International Vitreomacular Traction Study Group classificaton of vitreomacular adhesion, traction, and macular hole, Ophthalmology. 120, 2611– 2619 (2013).
- Haritoglou C., Ehrt O., Gass C.A., Kristin N. and Kampik A., Paracentral scotomata: a new finding after vitrectomy for idiopathic macular hole, Br. J. Ophthalmol. 85(2), 231–233 (2001).
- Nazari H., Modarres-Zadeh M. and Maleki A., Pharmacologic Vitreolysis, J. Ophthalmic. Vis.Res. 5(1), 44–52 (2010).
- Shi G.Y. and Wu H.L., Isolation and characterization of microplasminogen. A low molecular weight form of plasminogen, J. Biol. Chem. 263(32), 17071–17075 (1988).
- Udaondo P., Diaz-Llopis M., Garcia-Delpech S., Salom D. and Arevalo J.F., Microplasmin for vitreomacular traction, Ophthalmology. 117(9),1859–1860 (2010).
- De Smet M.D., Valmaggia C., Zarranz-Ventura J. and Willekens B., Microplasmin: ex vivo characterization of its activity in porcine vitreous, Invest. Ophthalmol. Vis. Sci. 50(2),814–819 (2009).
- Sakuma T., Tanaka M., Mizota A., Inoue J. and Pakola S., Safety of in vivo pharmacologic vitreolysis with recombinant microplasmin in rabbit eyes, Invest. Ophthalmol. Vis. Sci. 46(9), 3295–3299 (2005).
- Stalmans P., Benz M.S., Gandorfer A., Kampik A., Girach A., Pakola S. and Haller J.A., Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes, N. Engl. J. Med. 367(7), 606–615 (2012).
- Weinand F., Jung A., Becker R. and Pavlovic S., Spontaneous resolution of vitreomacular traction syndrome, Ophthalmologe. 106(1), 44–46 (2009).
- Odrobina D., Michalewska Z., Michalewski J., Dzięgielewski K. and Nawrocki J., Long term evaluation of vitreomacular traction disorder in spectral-domain optical coherence tomography, Retina. 31(2), 324–331 (2011).
- Wang Z., Lv X., Wu M., Xu W. and Rong A., Spontaneous resolution of idiopathic vitreo macular traction syndrome in a healthy young man, Int. J. Clin. Exp. Med. 8(7), 11718–11720 (2015).
- Yamada N. and Kishi S., Tomographic features and surgical outcomes of vitreomacular traction syndrome, Am. J. Ophthalmol. 139(1), 112–117 (2005).
- Carpineto P., Ciancaglini M., Aharrh-Gnama A., Agnifili L. and Mastropasqua L., Optical coherence tomography and retinal thickness analyzer features of spontaneous resolution of vitreomacular traction syndrome: a case report, Eur. J. Ophthalmol. 14(1), 67–70 (2004).