


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Dietary Practices and Factors That Can Influence the Outcome of a Pregnancy in Rural Communities in Nigeria
Nweze Nnakwe, PhD, RDN, LDN
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Adequate dietary intake is an essential component of ensuring a positive outcome. In Nigerian rural communities more than 87 percent of pregnant women have no access to any type of healthcare; the incidence of maternal and infant mortality is about 90 percent, due to hunger, poverty, malnutrition, iron deficiency anemia, and others. In addition, research on the dietary practices of pregnant women in rural communities in Nigeria is limited. Therefore, the purpose of this study was to examine the dietary practices, and factors that could influence the outcome of a pregnancy. Four hundred and fifty pregnant women enrolled in a community- based intervention program were recruited for the study. Data were collected from participants that volunteered using confidential questionnaire containing demographic characteristics, food frequency questionnaire, and information about factors that would influence the outcome of a pregnancy. The participants gave oral consent to participate in the study and received a note containing the name of a trained nurse they can contact for debriefing. Data was statistical analyzed using SPSS computer software. Results show that majority of the participant’s dietary intake from all the food groups was insufficient. Result also showed that factors that could negatively impact the outcome of a pregnancy exist in some of the participants. The difference between variables was statistical significant at p < 0.05. Sixty-two percent of the participants were not cognizant of prenatal nutrition counseling. Eighty-five percent reported irregular food intake and 15% ate regularly.
Prenatal care, Dietary Practices, Education Level
1. INTRODUCTION
Nutrition is one of the main factors in maternal and child health. Poor maternal nutritional status has been related to adverse birth outcomes; however, the association between maternal nutrition and birth outcome is complex and is influenced by many biologic, socioeconomic, and demographic factors, which vary widely in different populations [1-3]. In developing countries, other factors contribute to the high rate of maternal and infant mortality beside poverty. Some of these factors include limited access to healthcare facilities, shortage of transportation, little or no education, bad roads, no health education, and poor community support. In addition, the high rate of HIV infection compounds these problems in women [4, 5].
Exposure of the developing fetus to negative situations predisposes the fetus to various chronic diseases. Research studies have shown a link between maternal diet and neurological, immunological, and central nervous system development. These conditions contribute significantly in the subsequent development of mental disorders and other health conditions [2, 6, 7].
During pregnancy, women's dietary intake is considered an important factor in mother and fetus health. Adequate nutrients of different types are required to meet the increased demands of mother and the developing fetus [8]. Maternal dietary quality has been shown to be predictive of mental health problems in offspring. Even in the pre-conception period, maternal nutrition can have permanent and sustained phenotypic consequences for offspring [2]. This study aims to determine the dietary pattern of pregnant women and factors that may influence the outcome of a pregnancy.
2. Methods and Procedures
Four hundred and fifty pregnant women were recruited after they have enrolled in a community-based intervention program for a three-year period between the months of June and July. Data were collected from participants that volunteered using confidential questionnaire containing demographic characteristics, food frequency questionnaire, and information about factors that could influence the outcome of a pregnancy such as health conditions, education level, marital status, age, occupation, family income, and number of alive male and female children. The participants gave oral consent to participate in the study and received a note containing the name of a trained nurse they can contact for debriefing.
All statistical analyses were conducted using the Predictive Analysis Software for Windows (PAWS Statistics, version 18.0; SPSS Inc., Chicago, IL). Analyses conducted included descriptive analysis, and Pearson’s chi-square, between groups.
3. RESULTS
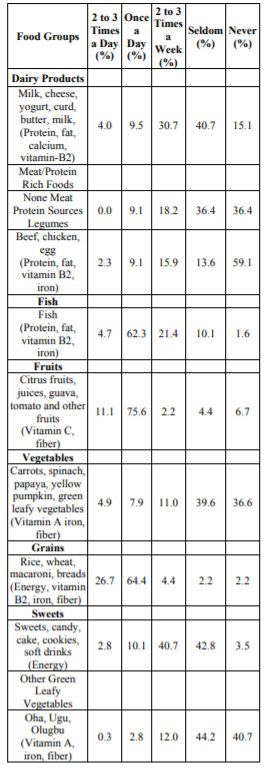
Table 1 contains the percentages of the food group intake of the participants. Results indicate that the participants were not consuming the recommended servings from every food group set by the USDA. The recommended serving size ranges for food groups were 6-11 grains, 2-3 vegetables, 3-4 fruits, 2-3 dairy foods, and 2-3 meat products. The findings from this study show that majority of participants, consumed bread and cereal, fruits, and fish at least once a day.
Majority of the participants relied less on meat as a source of dietary protein. Sixty-two percent consumed fish and meat 9.1% once a day. Eighty-five percent reported irregular meal pattern.
Result also showed that factors that could negatively influence the outcome of a pregnancy exist. These factors include anemia 32%, diabetes 35%, malaria 51%, hypertension 57%, and HIV infection 13%. In addition, sixty-eight percent of the participants were not cognizant of prenatal nutrition counseling. Furthermore, 70 percent of the participants had no plans to register for prenatal care or consult any health care professional.
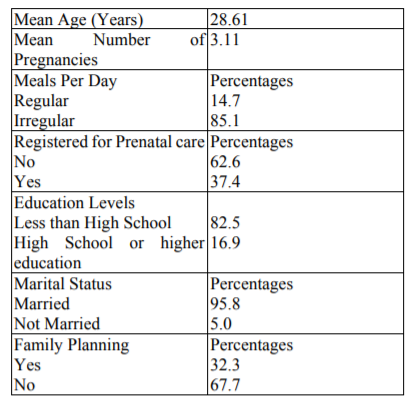
Table 2 shows that most of the participants had less than high school education. Significant association was found between consumption of meat, legume, milk and milk products, fruits and vegetables, and their educational level (p < 0.05). When participants were grouped according to marital status, 95 percent were married and only five percent was not married.
4. DISCUSSION
Pearson’s chi-square and descriptive analysis were used to determine the difference between groups listed in Tables 1 and 2. More than half of the women in this study were found to have nutrient intake insufficiency for all macronutrients and food sources for calcium, folate, iron and B vitamins. Factors associated with higher nutrient inadequacy were low educational, number of pregnancies and health conditions such as HIV, anemia, diabetes, malaria, and hypertension. There was a statistical significant difference between the groups at p< 0.05. Education was found to have a consistent effect all food groups consumption.
Nutrient intake is important to the well-being of pregnant women and the fetus. Inadequate nutrient intake can lead to maternal anemia, increasing the risk for other maternal morbidities and mortality, fetal growth retardation and low fetal birth weight [9, 10]. Inadequacy of macronutrient and micronutrient intake in pregnant women have been previously reported in developing countries [11-13].
Kramer, [14] observed that the countries which had achieved the lowest rates of adverse birth outcomes had done so not through health-care interventions but rather by reducing the prevalence of socioeconomic disadvantage. However, access to healthcare services in rural communities are lacking throughout Nigeria. Every year thousands of pregnant women and their children die from preventable health conditions such as iron deficiency anemia, diarrhea, lack of prenatal care, blood loss, home childbirth (many women in the rural area still give birth at home by untrained women), obstructed labor, malaria, eclampsia, placenta previa, and a variety of infectious diseases, including HIV infection [15, 16]. In these rural communities more than 87 percent of women have no access to any type of healthcare; the incidence of maternal and infant mortality is about 90 percent in addition to hunger, poverty, and malnutrition.
The women who survived, 15–20 women suffer short or long-term disabilities including obstetric fistulae (a hole between the vagina and rectum or bladder that is caused by prolonged obstructed labor, leaving a woman incontinent of urine or feces or both), ruptured uterus, paralysis and other complication [17].
5. CONCLUSION
Inadequate food intake was prevalent among pregnant women in this study. In addition, factors such education level, lack of prenatal care, and irregular meal pattern were observed. Sufficient nutrient intake is very essential during pregnancy because it influences fetal growth and birth outcomes. Most of the participants were not aware of prenatal nutrition counseling, nutrition education is a crucial component of prenatal care for a better outcome. The results of this study suggest that community or government support is needed in assisting poor pregnant women in Nigeria. There is a need to put more effort on good nutrition counseling at prenatal care clinics to increase nutrient intake, prevent malnutrition, and promote positive pregnancy outcome.
References
- Campbell, E., Gilliland, J., Dworatzek, P., and De Vrijer, D. , Socioeconomic status and adverse birth outcome: A population-based Canadian sample. . J. of BIO. SCI., 2018. 50(1): p. 102.
- Latal-Hajnal, B.,et al Postnatal growth in VLBW infants: Significant association with neurodevelopmental outcome. . J. Pedia., 2003. 143: p. 163-170.
- Irene, M., Bravo, M., Culture in Prenatal Development: Parental Attitudes, Availability of Care, Expectations, Values, and Nutrition..Child Youth Care Forum, 2014. 45: p. 521–538
- De Cock, K.M., Fowler, M.G., Mercier, E. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA 2000. 283(9).
- Huybregts, L.F., Roberfriod, D. A., Kolsteren, P. W., & Van Camp, J. H., Dietary behavior, food and nutrient intake of pregnant women in a rural community in Burkina Faso. Maternal and Child Nutr., 2009. 5(3): p. 211-222.
- Adrienne, O., Itsiopoulos, C., Skouteris, H. et.al., Preventing mental health problems in offspring by targeting dietary intake of pregnant women. BMC Med., 2014. 12: p. 208.
- Hendrik, J., Camp, V., Dietary behaviour, food and nutrient intake of pregnant women in a rural community in Burkina Faso. Maternal and Child Nutrition., 2009. 5: p. 211–222.
- Akhtar, S., et al, Prevalence of vitamin A deficiency in south Asia: Causes, outcomes, and possible remedies. . Health Pul Nutr., 2013. 3(4): p. 413-423.
- Brabin, B.J., Hakimi, M., and D. Pelletier., An analysis of anemia and pregnancy-related maternal mortality. J. of Nutr., 2001. 131: p. 604S-615S.
- Oguntona, C., and Akinyele, I.., Food and nutrient intakes by pregnant Nigerian adolescents during the third trimester. . Nutr., 2002. 18: p. 673-679.
- Sukchan1, P., Liabsuetrakul, T.,Chongsuvivatwong,V., and Songwathana. P., Inadequacy of nutrients intake among pregnant women in the deep south of Thailand. . BMC Pub. Health. , 2010. 10: p. 572.
- Capra, L., Tezza, G., Mazzei, F., Boner, A., The origins of health and disease: The influence of maternal diseases and lifestyle during gestation. J. of Pedia., 2013. 39: p. 7.
- Jacka, F.N., et al. , Maternal and early postnatal nutrition and mental health of offspring by age 5 years: A prospective cohort study. . JAM ACAD Child Adolescence Psychiatry 2013. 52: p. 1038–1047.
- Kramer, M., The epidemiology of adverse pregnancy outcomes: An overview. The J. of Nutr. , 2003. 133(5): p. 1592S-1596S.
- Ogundipe, S., & Obinna, C, Maternal death: Caging the terror of Nigerian women. . 2009.
- Smith, D., Unicef 'concerned over infant mortality rates in Nigeria'. Retrieved. 2010.
- World Health Organization, Maternal mortality. 2018.