


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Assessment of Low Birth Weight and Associated Factor among Neonate Delivered at Jimma University Medical Center (JUMC), Jimma Zone, Oromia Region, South–Western Ethiopia
Sheka Shemsi Seid1*, Adugna Dinsa1
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: Birth weight is sensitive indicator for predicting the chances for both infant survival and healthy child growth and development. LBW continues to remain major public health problem related to poverty, social factors such as lower status of women, malnutrition and lack of ANC.
Objective: To assess the prevalence of Low Birth Weight and associated factor, among the neonates born in Jimma university medical center from May 1, 2015 GC. to April 30,2017 E.C.
Methods: An institutional based retrospective cross sectional descriptive study was conducted on birth weight distribution. Data was collected by using structured data collection format from delivery registration book of obstetrics department and analysis was performed manually. Finally all the study result was presented by using tables, frequency, percentage, x2-test was employed to asses for association between variables.
Result: A total of 3546 singleton live- birth were observed among which 54% were male and 46% were female. The overall mean birth weight was 3200gm and the over prevalence of LBW was 6.7% statically the analysis showed that significant (p<0.05) independent effect on ANC follow up , gestational age, parity, sex of new born and maternal age during the last pregnancy while maternal residence, and seasons of delivery were not significantly related to low birth weight( p>0.05).
Conclusions: The prevalence of low birth weight in the study area was relatively lower than that of national figure. This is probably due to the improved health service delivery system as well as increased awareness of the community towards health service utilization. However this figure should not neglected as it is strong indicators of the health status of the community. There for the research still recommend expansion of ANC and health education particularly to reproductive age group to have awareness on maternal health care appropriate record keeping system and doing further studies on related issues.
birth weight, neonate, associated factor, Jimma, Ethiopia, Nursing and Healthcare
1. Introduction
Birth weight is the first weight of the new born obtained immediately after birth. For live birth it should be measured with in the first hour of life before significant post-natal weight loss occurred [1]. Birth weight is classified as macrosomia, normal birth weight and low birth weight (LBW) has been defined by the World Health Organization (WHO) as weight less than 2500 gram regardless of gestational age. This also further categorized into very low birth weight (VLBW), an infant birth weight less than 1500 g and extremely low birth weight (ELBW) is an infant weight less than 1000 g at birth regardless gestational age. The practical cut off international comparison is based on epidemiologic observation that infant weight less than 2500 gram is associated with high neonatal and infant morbidity and mortality of the estimated 4 million neonatal deaths. Preterm and LBW babies represent more than a fifth. Those who survive could have impaired immune function and increased risk of disease and are likely to remain malnourished (2, 1 and 3).
LBW children are also prone to have lower IQ and cognitive disabilities which affect their performance in school, job opportunities as adults and may develop chronic illness like diabetes and coronary heart disease in adult hood [1,2,4,5]
According to WHO technical consultation report on promoting optimal fetal development, birth weight of an infant is dependent on amount of growth during pregnancy and the gestational age, and these factors are related to the genetic makeup of the infant and the mother, her lifestyle and her status of health [20]
The weight of an infant at birth is an important milestone. Birth weight is recognized not only as a reliable index of intrauterine growth but also as pertinent determinant of the probability of infant surviving and experiencing as global indicators of the community health[6,10]
The global prevalence of LBW is 15.5 percent, which amounts to about 20 million LBW infants born each year, 96.5 percent of them in developing countries. Half of all low birth weight babies are born in South-central Asia where 27 percent are below 2500g at birth while LBW levels in sub-Saharan Africa are estimated at 15 percent [15]. Many of the report birth weight do not distinguish between LBW due to preterm delivery and LBW due to Intra Uterine Growth Restriction (IUGR). It is generally assumed that most of the excess prevalence of LBW in tropical countries is due to a higher frequency of IUGR. It was estimated that LBW due to IUGR is seven times higher in developing countries. While the rate of prematurely is only twice that of developed countries [8].
LBW is either the result of preterm birth or IUGR is known to cause cerebral palsy more frequent hospitalization for all illness, more hearing and visual disability more behavioral disorders. In habited growth and hearing problems when they enter school [1,2,10].
In Ethiopia reliable data on factors associated with birth weight are limited to few studies on LBW infants which was done mainly for the investigators. Therefore this study will be conducted pertaining birth weight distribution and to analyze the prevalence of LBW in this particular area.
2. Method And Material
The study was conducted in Jimma university medical center (JUMC) which is found in Jimma Town, Jimma Zone, Oromia Region and South-Western Ethiopia. Jimma Town has 346 Km from the capital city of Finfinne. Jimma university medical center which serves as a referral hospital for zonal hospitals and health centers in the zones has different departments among these obstetrics departments is the one under which delivery service for both normal and abnormal laboring mothers given caesarean section, instrumental delivery and spontaneous vaginal delivers. As per JUMC statistics, the center is currently providing different services for approximately 18 million people in the catchment areas. Maternity services are one of the wards with highest patient flow. Last year, the total number of live births was 3,976, among which 3,504 were live term births and the other 472 live Preterm births.
Two years retrospective cross sectional study was conducted from May 1, 2015 G.C. to April 30, 2017G.C.
No sample was drawn and all singleton live births in the study period were included.
Data were extracted by reviewing delivery registration book of Jimma university medical center and card of the study subject using a structured checklist adapted from previous related study[13]. The quality of the data collected was guaranteed by pretesting being done on 5% newborns medical records before actual data collection, and essential modifications then being made. The data was collected by diploma nurses after the training was given for them on how to collect on how to collect data from the records to augment data accuracy and validity. There was close supervision of data collectors by the investigators.
The Collected data were, cleaned, coded and entered into Epidata 3.1 entered and exported, to SPSS for windows version 23.0 for cleaning and analyses, data were summarized, by using simple frequency tables, graphs and charts. x2-test was done to, to determine the association between dependent and independent variables. Statically significant association was declared at p-value of 0.05
Ethical clearance to conduct the study was obtained from the institutional review board of the Institute of Health, faculty of Health Sciences, Jimma University. Further permission was obtained from the medical director of JUMC and the department head of pediatrics and gynecology for the utilization of medical records. We guaranteed confidentiality by excluding names or any other personal identifiers from data-collection sheets and reports. The identifier for each eligible subject was replaced by a code, and no master code exists that allows the research data to be linked with the identifiers.
3. Results
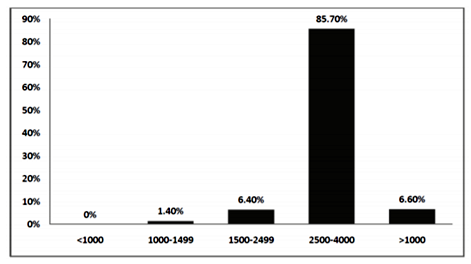
A total of 3546 singleton live births neonate were delivered at Jimma hospital during the period between May 1, 2015 G.C to April 30, 2017 G.C. Among these 1918 were male and 1628 were females. The overall mean birth weight was 32000 gram. The mean birth weight of male and female 3221 gram and 3175 gram respectively which showed that male was 46gm higher than that of the females. Of the total 3546 singleton live births 8% had less than 2500 g birth weight. and 85.7% were between 2500 gram and 4000 grams while 6.6% had greater than 4000gram birth weight (figure 1)
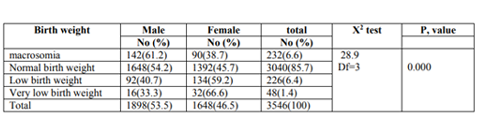
From normal birth weight more than half 1648 (54.2%) were male and Out of total LBW newborns majority 134(59.2%) were females.
Regarding VLBW majority 32(66.6%) were females. This finding showed that sex was found to be significantly associated with the birth weight (table 1).
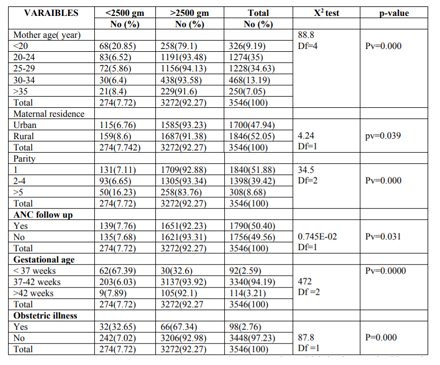
Out of those mother who gave birth of < 2500g newborn majority 83(30.3%) were aged between 20-24 years and followed by those mother aged between 25-29 which accounted 72(26.3%). Regarding maternal residence out of the total mothers 1700(47.2%) live in urban setting and 1846 (52.1%) in the rural area and the prevalence of low birth weight was 6.76% and 8.6% respectively. Maternal age and residence is found to be significantly associated with birth weight of the newborns (See table 2).
4. Discussions
The prevalence of LBW among the newborn delivered in JUMC was 7.8% and the normal birth weight was 85.7%. while the remaining was macrosomia. This finding is inconsistent with that of the national figure which is 16%[1,5,9]. This difference might be due to the fact that increased health service deliveries to achieve the goal of reducing low birth weight incidence at least by one third up to 2010 adapted by united nation general assembly special session on children on 2002[1] Another possible reason for lower low birth weight in our study area could be due to unreported home deliveries. This is evidenced by that of most labor of low birth weight is not difficult as compared to normal birth weight neonates.
This study showed that sex of the new born has significant association with birth weight of the newborns and also in this study males were 49 gram heavier than females. This finding was consistent the other similar study[13]. As usual low births weight all, more boys born than girls in every society which is also true in this study [3].
This study also revealed that the age of the mother is significantly associated (p< 0.05) with low birth weight). The available literature also support teenagers mother and those of age thirty five years above have higher rate of low birth weight than in their 20’s, and early 30’s [10].
This study also revealed that maternal parity was significantly associated (p< 0.05) with low birth weight. Similar to this finding the other study also revealed that as parity has a modest effect on birth weight. First born infant tend to be smaller and more often categorized as IUGR. This effects decrease with successive deliveries and it is not seen beyond the third [10].
The present study also showed that ANC and obstetric illnesses during the current pregnancy were associated with low birth weight. Neonates whose mother did not have ANC follow up higher prevalence low birth weight (7.76%) as compared to neonate whose mother had ANC follow up (7.68%). The possible explanation is that mother who had more ANC follow up have their obstetric problem detected and treated or referred earlier [3].
In this study gestational age of the mother has significant association with low birth weight (p< 0.01). Theoretically the shorter the gestation (the preterm births): the smaller is the baby and higher the risk of healthy and this finding is consistent with the study done in Jimma [3].
In conclusions the prevalence of low birth weight in the study area was relatively lower than that of national figure. However this figure should not neglected as it is strong indicators of the health status of the community. This study showed sex of the new born, parity, maternal residence, obstetric illness, during the current pregnancy and maternal age, ANC follow up and gestational age were found to have statistically significant effect on LBW.
Maternal and child health service such as family planning, ANC follow up service should be strengthened, so that the preventable and treatable case of LBW would be identified and treated earlier. Furthermore large scale research either hospital or community based must be cared out to get the clear picture of the problem and its risk factors for an appropriate design of intervention to reduce the magnitude of LBW in the study area.
References
- WHO, UNICEF.LBW country regional and global estimated report, 2004.
- Katharyn A, laura R, comprehensive maternity nursing second edition importance of nutrition during pregnancy pag 360-361
- UNICEF. LBW A tabulation of available information on the maternal health and safe motherhood program Geneva 1992 UNICEF
- Hindrics B, mattew R, pediatrics in topics fourth edition LBW and prematurity 1991 :198
- Kangaroo mother care, a practical guide department of RH and research Geneva WHO. 2003
- Ann K, Tassa W, monitoring LBW. The international J of public health march 2005:83(11):178-184
- Development of indicator for monitoring progress towards health for all by the year 2000” health for serious no 4 wtto. Geneva 1981.
- Nelson text book of pediatrics, 17th edition 2004:23
- Aseffa M, tesemma F, patterns of birth weight at community level in south west ethioipia. Ethio. J health science jan 2004 14(17):13-22
- Jones.WL, fundamentals of obstetrics and gynecology 8th edition 2005 edinburg London 27: 219-222
- MYLESS –text book for midwives 13th edition church liing stone 1999
- UNICEF, oxford university press the states of world children report, 1995.
- Fikre E, akililu M, chonge in birth weight of hospital delivered neonate in Addis Ababa. Ethiopia J. health dev 2004:14(18)
- Siza JE. Risk factors associated with low birth weight of neonates among spregnant Women attending a referral hospital in northern Tanzania. Tanzania Journal of Health Research. 2008; 10(1):1–8. 11.
- United Nations Children’s Fund and World Health Organization. Low Birth Weight: Country, regional and global estimates. NEW YORK: UNICEF; 2004.
- Kenya National Bureau of Statistics (KNBS) and ICF Macro. Kenya Demographic and Health Survey 2008-09. Calverton, Maryland: KNBS and ICF Macro; 2010.
- Agarwal K, Agarwal A, Agarwal VK, Agarwal P, Chaudhary V.Prevalence and determinants of “low birth weight” among institutional deliveries. Ann Nigerian Med. 2012; 5:48–52.
- Berihun M, Meseret Z, Nuru M, Incidence and correlates of low birth weight at a referral hospital in North West Ethiopia. Pan African Medical Journal. 2012; 12:4.
- Tema T, Prevalence and determinants of low birth weight in Jimma zone South West Ethiopia. East African Medical Journal. 2006;83(7):366–71
- World Health Organization. Promoting optimal fetal development Report of a Technical Consultation. Geneva, Switzerland: World Health Organization; 2006.