


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Acute Kidney Injury Due to Vitamin D Intoxication in a Body Builder
Dineshkumar T1*,Dhanapriya J1,Gopalakrishnan N1,Sakthirajan R1,Thirumurugan S1,Balasubramaniyan T1
Copyright : © 2017 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Body builders and professional athletes are widely using anabolic steroids, multi-vitamin and creatine supplements to increase their performance. Vitamin D overdose is one of the important causes of hypercalcemia. We report here a 21 years old male who was a professional weight lifter, presented with abdominal pain, polyuria and constipation. Investigations revealed acute kidney injury (AKI), hypercalcemia, hypervitaminosis D and low parathyroid hormone (PTH) level. Detailed history revealed intake of high dose of parenteral vitamin D for two months. He was treated intensively with intravenous saline, furosemide and steroids. Renal biopsy showed acute tubular injury and calcium concretions. His renal failure and calcium levels improved over weeks and laboratory parameters normalised at the end of two months.
acute kidney injury, hypercalcemia, intravenous saline, vitamin D,Nephrology
1. Introduction
Acute kidney injury in body builders is often due to volume depletion , rhabdomyolysis, nonsteroidal anti-inflammatory drugs usage , use of creatine supplements (interstitial nephritis/tubularatrophy)[1] steroids (acute interstitial nephritis).Apart from calcium homeostasis, vitamin D plays a role in improving muscle weakness, immunity and neuropsychiatric function. For improving muscle weakness and wellbeing, vitamin D supplements are being used without proper medical prescription[2]. Here we present a young male professional weight lifter who presented with AKI and hypercalcemia due to vitamin D overdosage and renal biopsy showed acute tubular injury and calcium concretions.
2. Case Report
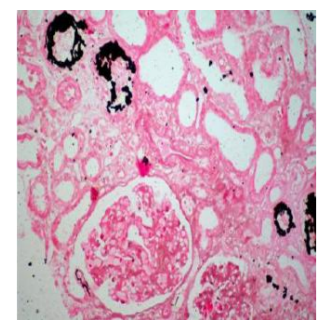
A 21 years old man was admitted with complaints of abdominal pain, polyuria, increased thirst, weight loss, fatiguability and constipation for 10 days. He was a non smoker, non alcoholic and weight lifter by profession. Examination revealed pulse rate:80/min;blood pressure:120/80 mmHg;body mass index : 23 kg/m2;body weight :65 kgs. Systemic examination was unremarkable. Investigations showed normal urinalysis; haemoglobin:11.8 G/dl; total leucocyte count: 7400/cu.mm; platelets :2.88 lakhs/ cu.mm; blood glucose :98 mg/dL;urea :65mg/dl; creatinine :3mg/dl; sodium :144 meq/L;potassium:4.2meq/L; corrected calcium: 15.56mg/dl; phosphorus :4.2mg/dl; magnesium:2mg/dl; uric acid: 6.6 mg/dl; LDH :250 U/L;CPK:44 U/L; total protein : 7.0 g/dl; albumin :3.8 g/dl; total bilirubin: 0.8 mg/dL; alanine transaminase :28 IU/L; aspartate transaminase: 32 IU/L; alkaline phosphatase:110 U/L.24 hrs urinary calcium was 209mg. Chest X-ray and electrocardiography was normal. Ultrasound of abdomen showed normal sized kidneys with a 4mm calculus in the midpole of right kidney. Serum PTH level was 7.04 pg/ml (15-65pg/ml) and 25(OH) vitamin D was more than 160 ng/ml. On repeated questions, he revealed intake of vitamin D (injection ARACHITOL) 12 lakhs units (2 ampoules) two times a week for 2 months with a cumulative dose of 192 lakhs units. He was also on calcium tablets and multivitamins. He denied usage of anabolic steroids and other nutritional supplements. Diagnosis of AKI secondary to hypercalcemia due to vitamin D intoxication was made. He was treated with continuous intravenous saline and frusemide. His peak creatinine was 3.1mg/dl. Our patient was having persistent hypercalcemia and renal failure and decline in calcium levels were not as expected, he was started on oral prednisolone 40 mg once daily (0.6mg/kg/day) at two weeks after admission. Renal biopsy showed acute tubular injury (figure 1) and calcium concretions in some of the tubules (figure 2). Serum calcium declined gradually. He didn’t require dialysis. At the end of 4 weeks after presentation, his creatinine was 1.1 mg/dl and corrected calcium was 11.5mg/dl. He received oral prednisolone 40 mg OD totally for 4 weeks followed by rapid tapering. At two months, his calcium was 9.9mg/dl and creatinine was 0.9 mg/dl.
Figure1: Renal biopsy showing acute tubular injury (H&E)
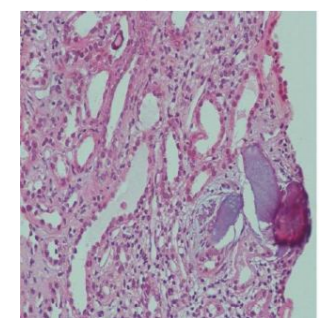
Figure2: Renal biopsy showing calcium concretions in the tubules (Von kossa)
3. Discussion
The recommended daily intake of vitamin D va-ries from 200 (children) to 600 IU (elderly). Pettifor et al[3]showed serum 25(OH)D levels in 11 patients with vitamin D toxicity ranged from 847 to 1,652 nmol/L with intake of higher doses of at least 20,000 to 30,000 IU per day.The clinical manifestations of vitamin D toxicity anorexia, polydipsia, constipation, abdominal pain, acute pancreatitis and peptic ulcer, polyuria, nephrocalcinosis and nephrolithiasis due to hypercalcemia and hypercalciuria, interstitial nephritis, acute and chronic renal failure, arrhythymia, short QT interval ,ectopic calcification, hypotonia, bony pain, confusion, and visual disturbances.
Hypercalcemia occurs as a result of intestinal calcium absorption/decreased renal clearance. Polyuria occurs because of decreased response to vasopressin in collecting ducts. Acute hypercalcemia impairs kidney function by causing direct renal vasoconstriction and by promoting hypovolemia [4]. Nephrocalcinosis is characterized by abundant renal tubular and interstitial deposits of calcium phosphate. The calcium deposits are associated with chronic, irreversible scarring in the form of tubular atrophy and interstitial fibrosis.
Elevated serum 25(OH)D level, normal 1,25(OH)₂ D level and depressed or normal PTH favors diagnosis of vitamin D intoxication Treatment consists of stopping of vitamin D intake, avoiding all calcium containing food in diet. Mild hypercalcemia needs no immediate treatment. Moderate hypercalcemia if symptomatic requires aggressive therapy. Severe hypercalcemia needs intensive therapy even without symptoms. The treatment include hydration with intravenous saline, loop diuretics, bisphosphonates, steroids and calcitonin. In severe hypercalcemia who present with coma, ECG changes and severe renal failure, hemodialysis with low or no calcium dialysate can be done[4].
Calcitriol induced hypercalcemia usually lasts for few days due to shorter half life. But overdose of preparations like dihydrotachysterol, vitamin D2 and D3 take longer time due to the deposition to fat and longer half life of 2-3 weeks. A case of AKI in a bodybuilder associated with use of veterinary substances containing vitamins A, D, and E with severe hypercalcemia due to synergestic effect of vitamin D and A was reported [5].Daher et al[6] reported two cases of hypercalcemia with acute kidney injury following intake of overdose of anabolic steroids along with vitamin D supplements.
Our patient presented with symptoms of hypercalcemia .On probing ,he admitted use of arachitol injections with cumulative dose of 192 lakhs units. He was treated with supportive measures without dialysis and recovered completely over two months. Detailed history helps in evaluation of hypercalcemia. Prognosis depends on the severity of illness and long term sequelae can be avoided with timely diagnosis and treatment. This case highlights the risk of AKI and probably chronic kidney disease in young men aspiring bodybuilding due to misuse of pharmacological drugs without proper prescriptions.
References
- Koshy KM, Griswold E, Schneeberger EE. Interstitial nephritis in a patient taking creatine. N Engl J Med 1999; 340: 814-5
- Koutkia P, Chen TC, Holick MF. Vitamin D intoxication associated with an over-the-counter supplement. N Engl J Med.2001; 345:66-7
- Pettifor JM, Bikle DD, Cavaleros M, Zachen D, Kamdar MC, Ross FP. Serum levels of free 1,25-dihydroxyvitamin D in vitamin D toxicity.Ann Intern Med. 1995;122:511-3
- Moyses-Neto M, Guimaraes FM, Ayoub FH, Vieira-Neto OM, Costa JA, Dantas M. Acute renal failure and hypercalcemia. Ren Fail. 2006;28:153-9
- Rocha PN, Santos CS, Avila MO, et al. Hypercalcemia and acute kidney injury caused by abuse of a parenteral veterinary compound containing vitamins A, D, and E. J Bras Nefrol 2011; 33: 467–71
- Daher EF, Silva Júnior GB, Queiroz AL et al. Acute kidney injury due to anabolic steroid and vitamin supplement abuse: report of two cases and a literature review. Int Urol Nephrol. 2009;41:717-23