


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
The Validity of the Hematocrit/Hemoglobin Ratio of 3.25 for the Diagnosis of the Alpha-Thalassemias
Somchai Insiripong1*,Tanarat Supattarobol1,Arunee Jetsrisuparb2
2.Division of Hematology, Department of Pediatrics, Faculty of Medicine, Khonkaen University, Khonkaen, Thailand.
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: The hematocrit (Hct) to hemoglobin (Hb) ratio is newly found to be 3.25 – 4.12 in alpha-thalassemias, instead of 3.0 as found in normal people.
Objective: To test the validity of the Hct / Hb ratio of 3.25 or more in the diagnosis of the alpha-thalassemias.
Patients and Method: Participants are the patients of clinical or hematological suspicion of thalassemia at the medical OPD, MaharatNakhon Ratchasima Hospital. From CBC, the Hct to Hb ratio of 3.25 or more is considered positive for the alpha-thalassemias and Hb analysis using HPLC method is used as the gold standard.
Results: From 300 participants, there are 130 with the alpha-thalassemias and 170 with non-alpha-thalassemias consisting of 101 with beta thalassemia / Hb E disease and 69 with Hb E disease. The test is found positive in 126 of 130 with the alpha-thalassemias and in 15 of 170 with non-alpha-thalassemias but negative in 4 of 130 with the alpha-thalassemias, 155 of 170 with non-alpha-thalassemia; 86 of 101 with beta thalassemia / Hb E, and all of 69 with Hb E disease. The sensitivity, the specificity, the positive predictive value, the negative predictive values, the positive likelihood ratio and the negative likelihood ratios of the tests are 96.9%, 91.2%, 89.4%, 97.5%, 11.0 and 0.03, respectively.
Conclusion: The Hct / Hb ratio of 3.25 or more is very powerful to distinguish the alpha-thalassemias from beta-thalassemia / Hb E and Hb E diseases in the cases of suspicious thalassemia.
Alpha-thalassemias, Hematocrit / Hemoglobin Ratio,Hematology
1. Introduction
The ratio of hematocrit (Hct) to hemoglobin (Hb) has been generally accepted to be 2.941 for long time[1], and it is simplified to be 3.0 in the daily clinical practice. This figure can be applied for the people who have normal red blood cell (RBC) morphology. In case of alpha-thalassemias, the patients always have microcytic, hypochromic, anisopoikilocytic RBC and their mean Hct to Hb ratio are newly found to be 3.5+0.2 (range 3.25 from 4.12) which is totally different from 3.02+0.08 (range 2.86 – 3.17) of the normal control[2]. The cause of the high Hct/Hb ratio among the patients with the alpha-thalassemias is supposed to be the effect of the uniform over-hydration of their RBCs while the RBCs of the patients with beta thalassemia / Hb E disease have heterogeneous hydration.
The diagnosis of the alpha-thalassemias which includes H, Hb H -Constant-Spring (CS), HbAEBart, HbAEBart-CS, HbEFBart and HbEFBart-CS diseases, is mostly made depending on the finding of the bands of Hb H and/or Hb Bart with or without Hb CS or Hb E from the various Hb analysis methods which may take a few hours or days to accomplish the test. If the figure of the high Hct/Hb ratio can be used to distinguish the alpha-thalassemias from other thalassemias and/or hemoglobinopathies with accuracy, it will be more convenient and more rapid for the clinicians to plan the management of the patients. This study is aimed to verify the validity of the Hct / Hb ratio at the cut point of 3.25 or more for the diagnosis of the alpha-thalassemias, viz. Hb H, H-CS, HbAEBart, HbAEBart-CS, HbEFBart and HbEFBart-CS diseases in patients with clinically and/or hematologically suspicious thalassemia.
2. Patients And Method
This cross-sectional study recruited the patients with 20 years of age or older who attended hematology clinic, department of medicine, Maharat Nakhon Ratchasima Hospital, with the clinical or hematological suspicion of thalassemia, i.e., chronic hemolytic anemia, hepatosplenomegaly, thalassemicfacy, low MCV, low MCH or the microcytic hypochromic anisopoikilocytotic red blood cell morphology on the peripheral blood smear. All patients were routinely investigated for CBC with the automated hematology analyzer (Sysmex, XT 1800i®) and the Hb analysis using the HPLC method (Bio-Rad instrument). The results of Hb analysis which was interpreted by the well trained medical technologist and the hematologist was used as the gold standard. The alpha-thalassemias included: Hb H, Hb H-CS, HbAEBart, HbAEBart-CS, HbEFBart and HbEFBart-CS diseases.
The value of Hct/Hb ratio was calculated from the CBC performed on the same day of Hbanalysis. The ratio of 3.25or more was used as the cut-off point to be positive for the alpha-thalassemias.
The patients who had concomitant chronic liver or kidney diseases, pregnancy, or the previous transfusion in less than 3 months were excluded. The study was approved by the ethical committee of Maharat Nakhon Ratchasima hospital.
3. Results
There were 300 patients with clinical or hematological suspicion of thalassemias. Their ages ranged from 20 to 81 years, mean 38.5 + 15.6 years. Males to females ratio were 125 to 175. Their means of Hb concentration, Hct, MCV and MCH were 8.0 + 2.7 g%, 25.9 + 8.2 %, 64.7 + 8.9 fl and 20.0 + 1.8 pg, respectively. From 300 patients, there were 130 with the alpha-thalassemias and 170 non-alpha-thalassemias which consisted of 101 with beta thalassemia / hemoglobin E disease and 69 with hemoglobin E disease. The overall mean Hct / Hb ratio was 3.260 + 0.368. The Hct/Hb ratio of 3.25 or more was found in 126 from 130 with the alpha-thalassemias and 15 in non-alpha-thalassemia group; all 15 found in beta-thalassemia /Hb E disease, none in Hb E disease group. It was found negative in 4 with the alpha-thalassemias, and in 155 with non-alpha- thalassemia; 86 with beta-thalassemia/Hb E disease and 69 with Hb E disease.
Of all 69 patients with Hb E disease, mean Hct/Hb ratio was 2.87+0.14, furthermore no one had the ratio close to 3.25 or nucleated red blood cell (NRBC).
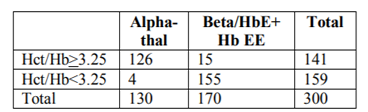
The sensitivity, the specificity, the positive predictive value (PPV), the negative predictive value (NPV), the positive likelihood ratio (PLR) and the negative likelihood ratio (NLR) were calculated to be 96.9% (95% Confidence Interval or CI: 92.3-99.1), 91.2% (95% CI: 85.9-95.0), 89.4% (95% CI: 83.1-93.9), 97.5% (95% CI: 93.7-99.3), 11.0 (95% CI: 6.8-17.8) and 0.03 (95% CI: 0.01-0.09), respectively.
From 126 alpha-thalassemia patients with positive test result, 5 had nucleated red blood cells (NRBC), ranging from 1 to 320 cells, median 6cells/100 WBC in the peripheral blood whereas none of the 4 alpha-thalassemia patients with negative test result had NRBC.
From beta-thalassemia/Hb E patients, all 15 cases with positive test result had NRBC, ranging from 2 to 480, median 132.5 cells/100 WBC whereas 14 from 86 with beta thalassemia /Hb E with negative test result (16.3%) had NRBC, ranging from 3 to 248 cells, median 51.0/100 WBC. The former had the NRBC much more than the latter with statistical significance (p-value < 0.0001).The rest of 72 with beta thalassemia / Hb E and all 69 with Hb E disease had no NRBC in the peripheral blood and negative test result.
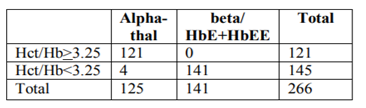
If the patients who had NRBC were all excluded from every group, the new contingency table could be yielded. The sensitivity, the specificity, the PPV, and the NPV of Hct/Hb ratio of 3.25 or more for the diagnosis of the alpha-thalassemias could be newly calculated after the patients with NRBC in any group were excluded as follows: 96.8%, 100%, 100%, and 97.2%, respectively.
4. Discussion
The Hct/Hb ratio of 3.25 or more can mostly distinguish the patients with alpha-thalassemias from beta-thalassemia/ Hb E and Hb E diseases with the high sensitivity, specificity, PPV and NPV. Probably because the alpha thalassemic RBCs are uniformly less dense than the normal while the beta thalassemic RBCs have a broad-density distribution. The less density of RBCs of alpha thalassemia may cause the falsely high Hct3 and the decreased Hb level compared with both decreased and increased Hb level of beta thalassemic RBCs[4].
All 15 beta thalassemia/Hb E patients with the positive test result have NRBC (100%) in the periphery and the rate of positive NRBC is significantly more common than 16.3 % of the beta thalassemi /Hb E group with negative test result. When the patients with positive NRBC from every group are excluded, the sensitivity, the specificity, the PPV and the NPV are changed from 96.9 %, 91.2 %, 89.4 % and 97.5 %, respectively to be 96.8 %, 100 %, 100 % and 97.2 %, respectively. This can be explained by the fact that the numerous NRBC which are more frequently found in beta-thalassemia/Hb E patients, may cause falsely high Hct determined by the automated hematology analyzer, resulting in high Hct/Hb ratio in some cases with beta thalassemia/Hb E disease[5].
Furthermore, when the Hct/Hb ratio of the alpha thalassemia-1 traits is calculated, it is also found high, 3.317 for males and 3.324 for females6. If it coincides with beta-thalassemia/Hb E, it may also cause the high Hct /Hb ratio in this group. This may be the underlying why a few cases of the beta thalassemia/Hb E patients have falsely positive test result. The role of the alpha thalassemia-1 hetrozygosity in cases of beta thalassemia/Hb E in this aspect needs to be clarified in the further study. Four of 130 cases (3.0 %) of the alpha-thalassemias have the negative test result without the proper explanation so far.
5. Summary
The Hct/Hb ratio of 3.25 or more has strongly diagnostic power to distinguish the alpha-thalassemias from beta-thalassemia/Hb E and Hb E diseases in the cases of suspicious thalassemia with the sensitivity, the specificity, the positive predictive value, the negative predictive value, the positive likelihood ratio and the negative likelihood ratio of 96.9%, 91.2%, 89.4%, 97.5%, 11.0 and 0.03.
References
- Weatherall MS, Sherry KM. An evaluation of the Spuncrit™ infra-red analyzer for measurement of haematocrit. Clin Lab Haem 1997; 19: 183-86.
- Insiripong S, Supattarobol T, Jetsrisuparb A. Comparison of hematocrit / hemoglobin ratios in subjects with alpha-thalassemia, with subjects having chronic kidney disease and normal subjects. Southeast Asian J Trop Med Public Health 2013; 44: 707-11.
- Schrier SL, Rachmilewitz E, Mohandas N. Cellular and membrane properties of alpha and beta thalassemic erythrocytes are different: implication for differences in clinical manifestations. Blood 1989; 74: 2194-202.
- Bunyaratvej A, Fucharoen S, Greenbaum A, Mohandas N. Hydration of red cells in alpha and beta thalassemias differs. A useful approach to distinguish between these red cell phenotypes. Am J ClinPathol 1994; 102: 217-22.
- Thomas L. Hematocrit (HCT). In: Thomas L, ed. Clinical laboratory diagnostics, use and assessment of clinical laboratory results. Frankfurt/Main: TH-Books-Verl.-Ges, 1998: 479-82.
- Pornpatkul M, Wasi P, Na-Nakorn S. Hematologic parameters in obligatory alpha-thalassemia. J Med Assoc Thai 1969; 52: 801-11.