


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Iron Deficiency Anemia during Pregnancy Predicts Poor Maternal Thyroid Status
Shahzad Ali Jiskani1,Siraj Muneer2,Noreen Atzaz3
Copyright : © 2017 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction: Iron deficiency anemia in pregnancy is very common and is associated with increased demand and utilization by fetus. Iron plays essential role in our body and has affects many physiological functions including thyroid function.
Patients and materials: This is a cross sectional study conducted at Department of Pathology, Pakistan Institute of Medical Sciences and was performed during period March to August 2017. 120 patients who are pregnant females with iron deficiency anemia and 125 patients as control who are pregnancy female with normal iron status and without anemia.
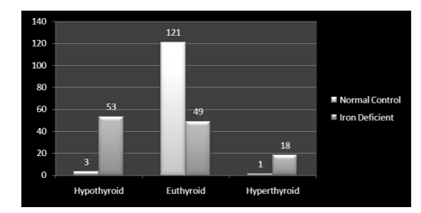
Results: Mean age of patients was 24.21 ± 21 years in normal pregnant females and 25.81 ± 3.1 years in iron deficient pregnant females. Mean gestational age in normal pregnant females was 28.32 ± 1.4 weeks, while in iron deficient pregnant female was 27.48 ± 2.3 weeks. In normal pregnant female patients, 3 (2.47%) were hypothyroid, 121 (96.8%) were euthyroid and 1 (0.8%) was hyperthyroid, while in iron deficient pregnant females, 53 (44.16%) were hypothyroid, 49 (40.88%) were euthryoid and 18 (15%) were hyperthyroid. There was a statistically significant difference of thyroid status in both groups (p < 0.001).
Conclusion: Iron deficiency was strongly associated with deranged thyroid status. So iron therapy is necessary to maintain thyroid status as they both have effects on each other.
Iron deficiency anemia, pregnancy, thyroid, fetus,Hematology
1. Introduction
Iron deficiency anemia is the most common nutritional deficiency among all micronutrients problems. Iron deficiency has many adverse effects in all age groups. In older children and adults, it decreases the capacity and output of work and disturbs the immune system. It is also associated with decreased reproduction capacity. Iron deficiency shows to have effects on heme – dependant enzymes which lead to multiple functional failures. Iron deficiency, being more prevalent during gestational age due to increased utilization or iron, creates more problems as compared to other age populations [1]. Pregnancy has clear effects on thyroid hormones and their function. Thyroid gland shows 10% enlargement during pregnancy in iodine – stuffed countries and 20 – 40% in areas with iron insufficiency. Production of triidothyronine (T3) and thyroxine (T4) also increases by 50% in addition to increased daily requirement of iodine. There is also a prominent increase in thyroxin – binding globulin (TBG) due to stimulation of thyroxin – binding globulin (TBG) production by increased maternal estrogen levels and decreased clearance by liver because of sialylation induced by estrogen. This will cause an enlargement of extra – thyroidal pool, ultimately leading to increase in total T3 and T4 concentrations [2]. These changes may cause hypothyroidism in later parts of pregnancy in females who are iodine – deficient [3]. Iron deficiency can disturb synthesis of thyroid hormone by decreasing plasma T3 and T4 concentrations due to impairment of two initial steps which are catalyzed by enzyme heme – dependent thyroid peroxidase (TPO) in the synthesis of thyroid hormone. There is also a decreased TSH response to TRH, reduction in peripheral conversion of T4 to T3 as well as increase in circulating TSH [4]. This study helps to see the correlation between iron deficiency during pregnancy and maternal status of thyroid hormones.
2. Patients And Methods
This is a cross sectional study conducted at Department of Pathology, Pakistan Institute of Medical Sciences Islamabad during the period of March to August 2017. Total of 120 patients were selected for the study which included pregnant females with iron deficiency anemia. 125 patients were taken as control which included pregnant females without iron deficiency anemia. Age in both groups ranged between 18 years to 35 years. All patients with drug history, sepsis, diabetes mellitus, hyper tension, history of iron supplementation or known thyroid disorder were excluded from the study. Criteria were made to describe iron deficiency anemia. A serum ferritin concentration of less than 20 µg/L and hemoglobin levels less than 11g/dL was considered as iron deficiency anemia. Blood samples from all patients were taken into two tubes. Samples collected in Gel tube were evaluated for serum TSH, T3 and fT4. The thyroid status was classified according to American Thyroid Association guidelines. It includes Hypothyroidism (increased TSH along with reduced fT4), subclinical hypothyroidism (increased TSH along with normal fT4), hyperthyroidism (reduced TSH along with increased fT4) and subclinical hyperthyroidism (reduced TSH along with normal fT4).
Data were analyzed and evaluated using SPSS version 21.0. P –value of < 0.05 was considered statistically significant.
3. Discussion
Iron deficiency is known as a common public problem having high prevalence and affecting approximately 2 billion people globally [5]. Pregnant females are more vulnerable to iron deficiency due to increased demand by fetus. Iron is an important micronutrient for our body and its deficiency leads to change in many physiological and metabolic reactions. Deficiency of iron leads to various problems including derangement of cognitive function, behavioral changes, immunity defects, thermoregulation problems and reduced work capacity. [6]. Additionally, iron deficiency anemia is a severe outcome of iron deficiency and is the most common type of anemia [7]. Abundant and convincing scientific data have revealed that iron deficiency anemia during pregnancy is associated with a wide range of dangerous perinatal and maternal consequences including preterm birth, low birth weight of fetus and poor neurological development of fetus.. It is also clear that iron stores in neonate can be affected when mother is suffering from iron deficiency anemia [8]. It is also now postulated that deficiency of iron with or without anemia affects metabolism of thyroid. It decreases plasma T3 and T4 levels, decreases the peripheral conversion of T4 to T3 and increases TSH concentration in plasma [2]. So Iron deficiency is a probable factor in the development of endemic goiter. Though, the exact mechanism is not clear. Iron deficiency is responsible for derangement of thyroid metabolism by affecting and making changes in the common hypothalamic–pituitary–thyroid (HPT) axis, thereby decreasing the adherence of T3 to hepatic nuclear receptors or possibly due to anemia and decreased transport of oxygen [9]. Iron deficiency also affects the hepatic activity of T4 – 5.
Deiodinase which is the enzyme responsible for converting T4 into T3 or the function of thyroid peroxidase which is responsible for synthesis of thyroid production, as it is iron – dependant [10]. Meanwhile, the supplementation of iron therapy recovers function of thyroid. Some intervention trials were conducted and proved that supplementation of iron significantly improves the performance of iodized oil and salts in pediatric patients with goiter. Iron therapy in females suffering from subclinical hypothyroidism also showed slight elevation of T4 and minor reduction in TSH levels. However, hypothyroidism itself is also responsible for various hematological defects as various mechanisms are involved in the development of these problems. Iron deficiency anemia maybe caused by poor absorption by intestine associated with deficiency of thyroid hormone or related gastic achlorhydria. Hence, supplementation with thyroxine is very important [6,11].
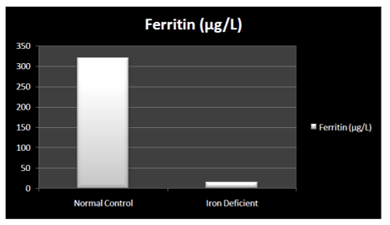
In the present study, it was postulated that thyroid status was deranged in pregnant women with iron deficiency. Hemoglobin and ferritin level was significantly different in iron both groups (Table 1, figure 1 and 2).
Table1: Baseline Parameters in both Groups (N=245)
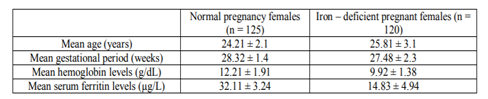
Figure 1: Hemoglobin difference in both groups (n=245)
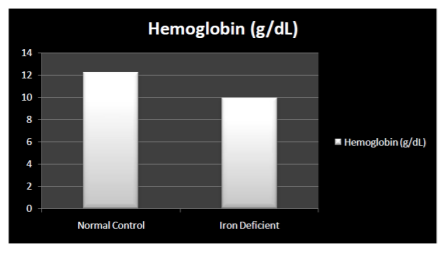
Figure 2: Ferritin difference in both groups (n=245)
Most of the patients with iron deficiency anemia were related with hypothyroidism, followed by euthryoid. While in normal control group very minor percentage of patients had deranged thyroid status (Table 2, figure 3).
There was a statistically significant difference in parameters in both group, suggesting the strong correlation between iron deficiency and thyroid status.
Table2: Thyroid Status in both Groups (N=245)

Figure 3: Thyroid status in both groups (n=245)
4. Conclusion
In current study, iron deficiency was strongly associated with deranged thyroid hormone functions. So proper diagnosis and management is very essential to overcome this deficiency as it can cause dangerous effects on mother as well as fetus.
References
- Eftekhari MH, Keshavarz SA, Jalali M, Elguero E, Eshraghian MR, Simondon KB. The relationship between iron status and thyroid hormone concentration in iron-deficient adolescent Iranian girls. Asia Pac J Clin Nutr. 2005;15(1):50–5.
- Sahay RK, Nagesh VS. Hypothyroidism in pregnancy. Indian J Endocrinol Metab. 2017;16(3):364–70.
- Stagnaro-green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, Nixon A, Pearce EN, Soldin OP, Sulivan S, Wiersinga W. Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease. Thyroid. 2011;21(10).
- Yu X, Shan Z, Li C, Mao J, Wang W. Iron Deficiency , An Independent Risk Factor for Isolated Hypothyroxinemia in Pregnant and Nonpregnant Women of Childbearing Age in China. J Clin Endocrinol Metab. 2017; 100(4): 1594–601.
- Scholl TO. Iron status during pregnancy : setting the stage for mother and infant. Am J Clin Nutr. 2005;81((suppl)):1218–22.
- Zimmermann MB. The Influence of Iron Status on Iodine Utilization and Thyroid Function. Annu Rev Nutr. 2006;26:367–89.
- Article O. The Role of Iron Deficiency in Persistent Goiter. Arch Iran Med. 2008; 11(2): 157–61.
- Zimmermann MB, Burgi H, Hurrell RF. Iron Deficiency Predicts Poor Maternal Thyroid Status during Pregnancy. J Clin Endocrinol Metab. 2017;92(9):3436–40.
- Khatiwada S, Gelal B, Baral N, Lamsal M. Association between iron status and thyroid function in Nepalese children. Thyroid Res. Thyroid Research; 2016;9(2):1–7.
- Veltri F, Decaillet S, Kleynen P, Grabczan L. Prevalence of thyroid autoimmunity and dysfunction in women with iron deficiency during early pregnancy : is it altered ? Eur J Endocrinol. 2016;175:191–9.
- Shuxiang L, Xin G, Yancai W, Gengchao Z, Chen Y. The Relationship between Iron Deficiency and Thyroid Function in Chinese Women during Early Pregnancy. J Nutr Sci Vitaminol. 2016;62:397–401