


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Cervical Cancer Diagnosed During the Third Trimester of Pregnancy
Yasmina Jose Gutierrez1*, Laura Baquedano Mainar1, Marta Lamarca Ballestero1, Silvia Ortega Marcilla1, Miguel Angel Ruiz Conde1
Copyright : © 2018 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cervical cancer during pregnancy is very uncommon and the mean age at diagnosis is 15 years less than the average age in general population. Although pregnancy is an excellent opportunity for detection of preneoplastic lesions and tumors in the early stages, several studies have shown that 76% of the lesions diagnosed during pregnancy are in stage IB.
There is no standard therapy and anagement should be individualized according to the clinical stage, gestational age and the patient’s desire.
We present a case of diagnostic and treatment of invasive carcinoma, stage IB2 diagnosis in a woman at 28 weeks of gestation.
Cervical Cancer, Pregnancy, Chemotherapy,Gynecology, Obstetrics
1. Introduction
Cervical cancer is the tumor with higher incidence and mortality in women after breast cancer around the world. 83% of cases occur in developing countries, and it is less common in countries with more resources. Spain is among the European countries with a lower incidence, but continues to be an unresolved issue since despite the campaigns of screening with a high fill, die every day in our country two women for this type of cancer. After breast and hematologic cancers, cervical cancer is one of the most common malignancies during pregnancy and the incidence rates vary from 1-15 cases per 10.000 pregnancies [1].
Pregnancy is a good time to start or upgrade screen for cervical cancer in patients without routine gynaecologic checkups. In order to unify the guidelines on the prevention of cervical cancer in Spain, the Spanish Society of Gynecology and Obstetrics (SEGO) has developed a guide to clinical practice, published in 2014 [2].
Treatment in a pregnant patient with cervical cancer needs to be individualized an several issues are important like histological subtype, disease stage, nodal status, gestational age and obstetrical complications and desired preservation of the pregnancy, for this reason standardization of treatment is very difficult. Inhis situation of special vulnerability for women is important to make a proper advice based on current clinical guidelines, innovations and controversies [3-5].
We report the management of pregnant women with stage IB2 cervical cancer. She received chemotherapy during pregnancy, and a TaxolCisplatin combination was used. By now, the women have no evidence of disease, and the infant demonstrate normal neuropsychomotor development.
2. Case Report
31-year-old patient pregnant of 28 weeks, referred to our service of Gynecology by genital bleeding and cervical mass suggestive of malignancy. The anamnesis did not reveal the presence of any antecedent or surgical physician interest. Gravid 1, para 0, gestation after in vitro fertilization. Prior to the current Pap smear was performed 18 months before.
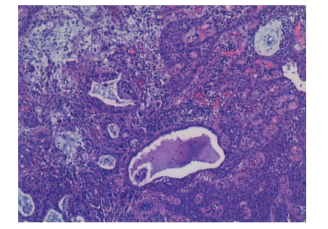
Pelvic examination revealed a 4cm exophytic cervical mass without vaginal or parametrial involvement. Biopsy of the mass revealed moderately differentiated adenocarcinoma of cervix. (Figure1).
We performed the following tests:
1. Transvaginal Ultrasound: 4-5 cm cervical mass.
2. Abdomino-pelvic Ultrasound: without pathological findings. confirmed the gestational age and excluded fetal abnormality and
3. Complete blood count, biochemistry and coagulation study: normal. Syphilis, Hepatitis B, Hepatitis C and HIV serologic test results are negative.
4. MRI confirmed a bulky mass of 44x35x36mm without parametrial involvement. No bladder or rectal involvement and no suspicious adenopathies (Figure2).
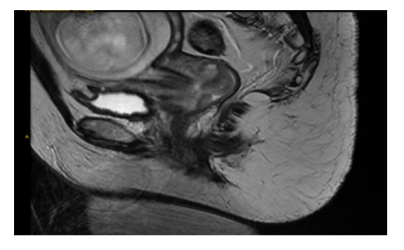
The tumor was classified as FIGO stage IB2.
We informing the patient of the histopathological result and extension study, the patient refused to terminate the pregnancy. After extensive discussion, she signed the consent form and elected neoadjuvant chemotherapy.
She received Paclitaxel 75 mg/m2 plus cisplatin 50 mg/m2 two times a week, but in the 29+6 weeks the patient had a worse ring of the general condition and heavy vaginal bleeding so it was decided according to the patient to end the pregnancy by cesarean section.
The newborn boy, weighing 1,290 g, had an Apgar score of 6, 9 and 10 at 1, 5 and 10 min, respectively. After recovering from the intervention the patient received pelvic
radiotherapy at a dose of 46 Gy with concomitant cisplatin chemo-sensitization.
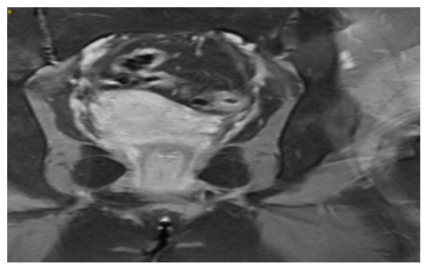
MRI six months after the end of treatment showed a complete response (Figure3).
After 5 years of finish treatment the mother has no evidence of local or distal relapse, and his infant is in good general condition.
3. Discussion
However the majority of cervical cancers diagnosed during pregnancy are in the early stages (76% in stage I cases), pregnancy can mask cancer related symptoms with delay diagnostic and higher stages when cancer is diagnosed. Our patient had a bulky mass greater than 4 cm despite having a negative Pap smear result was performed 18 months before. Karam et al. say pregnancy is an opportunity to screen for cervical cancer in patients without routine gynaecologic checkups [6-8].
Owing to the rarity of cervical cancer associated with pregnancy, definitive management guidelines for these patients remain unclear. Treatment depends on whether the patient desires to continue her pregnancy, as well as on the stage of the disease and gestational age at diagnosis [9].
The diagnosis of this disease during pregnancy always raises a number of ethical and therapeutic considerations that gestational age at diagnosis, stage, tumour size and genes desire are fundamental. Advice and treatment must be done with a multidisciplinary team and individually depending on the circumstances of each case [10-12].
There is evidence of retardation in the treatment of squamous cell carcinoma of the cervix in early stage is not likely to have a negative effect on the mother and that it could be extended to achieve fetal maturity, however the histologic subtypes of adenocarcinoma clear cell, small cell carcinoma or adenosquamous carcinoma have a faster growth than make recommended not to delay the start of the treatment [13,14] so in our case it was decided to start with neoadjuvant chemotherapy.
Neoadjuvant chemotherapy could be administered to reduce the tumor bulk, control micro metastatic disease and allow for fetal maturation [15]. Because its inhibition of tumor metastasis, it might be of particular value during pregnancy. Furthermore, complete and partial response has been reported in pregnant women with cervical cancer suggesting it be a reasonable choice for these patients [16].
Cisplatin is the most active agent in cervical cancer and it also has been used as an effective neoadjuvant chemotherapeutic regimen. A meta-analysis including 2,047 patients with cervical cancer showed that neoadjuvant chemotherapy lasted 14 days or less or cisplatin dose intensity of at least 25 mg/m2 per week was associated with a survival advantage [17].
Neoadjuvant chemotherapy with paclitaxel plus cisplatin appears to be feasible and safe for pregnant patients with invasive cervical cancer and infants. However, the drugs involved are potent teratogens and should be avoided during the first trimester. The main fetal effects from administration of therapeutic agents during the second and third trimesters relate to low birth weight (observed in 40% of the exposed neonates), intrauterine growth restriction, prematurity and intrauterine fetal death. Furthermore, chemotherapy should not be performed beyond 35 weeks of gestation, since delivery may occur during the period of greatest fetal immunosuppression [18]
In cases of invasive carcinoma detected up to the 12th week of pregnancy, patient treatment is the priority. When a diagnosis is made in the second trimester, it is possible to wait until fetal pulmonary maturity. Many recent studies have indicated the use of chemotherapy in order to stabilize the disease until the time of delivery, which should preferentially be by cesarean section [19].
References
- Al-Halal H., Kezouh A., Abenhaim H. Incidence and obstetrical outcomes of cervical intraepithelial neoplasia and cervical cancer in pregnancy: A population-based study on 8.8 million births. Arch Gynecol Obstet, 2013, Volume 287, Issue 2, pp 245–250.
- Oncoguía SEGO: Prevención del Cáncer de Cuello Uterino 2014. Gu ías de práctica clínica encáncerginecológicoymamario. Publicaciones SEGO, octubre 2014. Oncoguías ISBN: 978-84-612-7418-2
- Oncoguía SEGO: Cáncer de Cuello Uterino 2013. Gu ías de práctica clínica en cáncer ginecológico y mamario. Pub licaciones SEGO, octubre 2013. Oncoguías ISBN Vo l. 1: 978-84-612-7418-2.
- Ferlay J, Sh in HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010; 127: 2893-291.
- Castellsagué X, Remy V, Pu ig- Tintoré LM, Sain z de la Cuesta R, González Rojas N et al. Ep idemio logy and costs of screening and management of p recancerous lesions of the cervix in Spain. J Low Genit Tract Dis. 2009; 13:38-45.
- Sileny N. Han, M ina Mhallem Gziri, Kristel Van Calsteren and Frédéric A mant. Cervical cancer in pregnant women: t reat, wait or interrupt? Assessment of current clinical guidelines, innovations and controversies . Ther Adv Med Oncol. 2013 July; 5(4): 211–219.
- Karam A, Holschneider CH. Cervical cancer in pregnancy. UpToDate, Basow DS, ed itor, UpToDate, Waltham, MA, 2010.
- Sellerest L. Mathevet P. Precancerous cervical lesions during pregnancy: diagnostic and treatment. J Gynecol Obstet Biol Reprod 2008.
- Cortés J. Prevención primaria y secundaria de los cánceres de cuello de útero y vulva: recomendaciones para la práctica clínica . Prog Obstet Ginecol 2010; 53(supl 1):1-19.
- Cáncer de cérvix y embarazo. Protocolos asistenciales en Obstetricia. Reco mendaciones españolas revisadas 2008. Sociedad Española de Ginecología y Obstetricia (SEGO). Disponible en: www.prosego.com.
- Petterson BF, Andersson S, Hellman K, Hëllstrom A C. Invasive carcino ma of the uterine cervix associated with pregnancy: 90 years of experience. Cancer. 2010; 116(10):2343-9.
- Favero G, Chiantera V, Oleszcuk A, Gallota V, Hertel H, Herrmann J, et al. Invasive cervical cáncer during pregnancy: laparoscopic nodal evaluation before oncologic trat ment delay. Gynecol Oncol. 2010; 118(2):123-7.
- Lee JM , Lee KB, Kim YT. Cervical cancer associated with pregnancy: results of mu lticenter retrospective Korean study (KGOG-1006). A m J Obstet Gynecol. 2008; 198:92.
- Adriaensen WJ, Mathei C, Buntin x FJ, Arbyn M. A framework provided an outline toward the proper evaluation of potential screening strategies. J Clin Ep idemio l 2013 Jun; 66(6):639-47.
- Halaska MJ, Rob L, Robova H, Cerny M. Treat ment of gynecological cancers diagnosed during pregnancy. Future Oncol 2016, 12(19):2265-2275.
- Jing Li, Li-juan Wang, Bing-zhong Zhang. Neoadjuvant chemotherapy with paclitaxel plus platinu m fo r invasive cervical cancer in pregnancy: two case report and literature review. A rch Gynecol Obstet (2011) 284:779– 783.
- Timotheadou E, Gore M E (2003) Neoadjuvant chemotherapy fo r locally advanced cervical cancer. Eur J Cancer 39(17): 2419–2421.
- Pushpa Naga CH; Lavanya Gu rram; Supriya Chopra; Umesh Mahantshetty. The management o f locally advanced cervical cáncer. Current Opin ion in Oncology. 2018, 30(5):323– 329.
- Ngu, S.F., Ngan, H.Y. Chemotherapy in pregnancy. Best Pract. Res. Clin . Obstet. Gynaecol. 2016 May; 33:86–101.