


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Pancreatic Congenital Anomaly as a Cause of Acute Recurrent Pancreatitis in an Adult Patient
Maddalena Zippi1*, Chiara Marzano1, Wandong Hong2, Sirio Fiorino3, Giuseppe Occhigrossi1
2.Department of Gastroenterology and Hepatology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, China.
3.Unit of Internal Medicine, Maggiore Hospital, Local Health Unit of Bologna, Bologna, Italy.
Copyright : © 2018 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Pancreas divisum is a rare congenital malformation. It is generally asymptomatic and only 5% of patients present symptoms, such as acute recurrent pancreatitis. We describe the case of a 61-year-old man who came to our observation for acute pancreatitis due to a pancreas divisum. The patient has been successfully endoscopically treated by the sphincterotomy of the minor papilla.
acute recurrent pancreatitis, magnetic resonance cholangiopancreatography (MRCP), minor papilla (MiP), minor papilla sphincterotomy (MiES), pancreas divisum, Santorinicele, Gastroenterology
Case Report
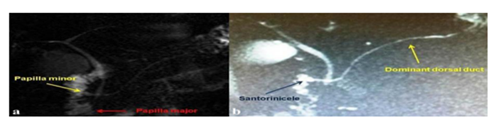
A 61-year-old has undergone to our observation for pancreatic abdominal pain. On admission, the blood chemistry tests showed more than 3-fold raised in pancreatic enzymes, while no indices of cholestasis or hepatic cytolysis were present. An abdominal ultrasound revealed a pancreas increased in volume and dishomogeneous, without local or extra-local complications, letting argue an episode of mild acute pancreatitis (AP) occurred. The patient was treated with bowel rest, broad spectrum antibiotics and gabexatemesilate until the normalization of the pancreatic function. A clinical interview was conducted, from which it emerged that the patient was hospitalized for another 2 episodes of AP in the last 3 years. A diagnosis of acute recurrent pancreatitis has been formulated. From both letters of discharge, AP was termed “idiopathic”. A magnetic resonance cholangiopancreatography (MRCP), performed at our Center, was very suggestive for a pancreas divisum (PD) (Figure 1a). As the main indication for minor papilla sphincterotomy (MiES) is strongly recommended for patients with symptomatic PD and signs of obstruction to outflow from the minor papilla (MiP), a dynamic MRCP after secretin stimulation was carried out (Figure 1b). The latter one confirmed the presence of a complete pancreas divisum with a dominant dorsal duct associated with a Santorinicele. The patient underwent a "pull type" MiES of the minor papilla (MiP), using appropriate sphincterotomy, without any intra or post-procedural complications. After one year of follow-up, the patient is still asymptomatic.
Pancreas divisum (PD) is an anatomical variant of the pancreatic duct system due to a failure of fusion of dorsal and ventral pancreatic portions during the embryogenetic process [1]. PD is reported in approximately 8% to 12.6% of the Western population, according to autopsy series [2] and in about 4-8% in the Western populations and less than 2% in the Asians during endoscopic retrograde cholangio-pancreatography (ERCP)[3]. Most of the time, PD is just an occasional finding, so much so that only less than 5% of patients develop symptoms[4]. The first description of an endoscopic approach to this condition dates back to 1978 by Professor Cotton, who first sensed that it was necessary in these cases decompressing the dorsal duct by favoring the pancreatic drainage [5]. It is widely recognized that the main indication to performa minor papilla sphincterotomy (MiES) is in a patient with symptomatic pancreas divisum and signs of obstruction to outflow from the MiP [6].
References
- DiMagno MJ, Wamsteker EJ. Pancreas divisum. CurrGastroenterol Rep. 2011;13(2): 150-6
- Dawson W, Langman J. An anatomical-radiological study of the pancreatic duct pattern in man. Anat Rec 1961; 139: 59-68
- Burtin P, Person B, Charneau J, et al. Pancreas divisum and pancreatitis: a coincidental association? Endoscopy 1991; 23:55-8
- Saltzman JR. Endoscopic treatment of pancreas divisum: why, when, and how? GastrointestEndosc 2006; 64:712-5
- Cotton PB. Duodenoscopic papillotomy at the minor papilla for recurrent dorsal pancreatitis. Endosc Digest 1978; 3: 27-8
- M. Zippi, P. Familiari, G. Traversa, I. De Felici, I. Febbraro, G. Occhigrossi, C. Severi. Role of endoscopic sphincterotomy of the minor papilla in pancreas divisum. ClinTer 2014; 165 (4):e312-316