


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Gastrointestinal Motor Function in Diverticular Disease
Lychkova A.E1*, Golubev Yu.Yu2, Severin A.E3, Puzikov A.M1
2.Russian National Research Medical University, Moscow, RF.
3.Peoples' Friendship University, Moscow, RF.
Copyright : © 2018 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Aim: The aim is to determine changes in gastrointestinal motor function in diverticular disease.
Materials and Methods: 22 patients with diverticulosis and 16 patients with diverticulitis were examined. The frequency and amplitude of electromotor activity (EMA) slow waves were recorded by the hardware-software complex Conan-M via surface contact bipolar electrodes applied to the projections of the stomach, the ascending, and descending parts of the colon to the abdominal surface.
Results and Conclusion: In diverticulosis hyper motor dyskinesia of the stomach and hypo motor dyskinesia of small and large intestines were diagnosed. In diverticulitis there were a hyper motor dyskinesia of biliary tract, small intestine, and descending part of the colon.
electromotive activity, disorders of gastrointestinal motor function, diverticulosis, diverticulitis, clinical study, Gastroenterology
1. Introduction
The state of the gastrointestinal motor function (GI) in diverticular disease may be examined by the analysis of the electromotive activity of its smooth muscles. Electromotive activity (EMA) is a combination of electrophysiological and related biochemical phenomena in the smooth muscle tissue. The EMA is characterized by the presence of slow waves, reflecting depolarization and repolarization processes. Muscle contraction occurs when there are significantly expressed amplitude characteristics of slow EMA waves and/or there is a spike activity. Direct electromyography is the most accurate method of recording electrical potentials. However, this method is not always convenient because of its invasiveness.
In this regard, in 1952-1954, Sobakin M.A. developed a technique for recording the gastric electrical potentials from the body surface (from the anterior abdominal wall in the projection of the position of the stomach). In 1974 Rebrov V.G. modified this method. He was the first to record the gastrointestinal electrical potentials from patient’s limbs [7]. Rebrov suggested the classification of electrical signals recorded in the GI frequency range. Similar results on the gastric frequency were also obtained by other researchers [2].
These data served as a basis for the algorithm of the intestinal electrophysiological activity assessment on the basis of its frequency characteristics and the creation of a peripheral electromyography method. The magnitude of the transmembrane potential was found to range from 20 to 90 mV. It can vary under the influence of various effects such as hormonal, nervous, mechanical, temperature and, in particular, chemical [5].
There are three variants of the gastric electrical activity[5] :
Normagastria: The maximum electrical activity of the stomach falls in the frequency range of 2-4 cycles/min.
Bradygastria: The maximum electrical activity of the stomach falls in the frequency range of < 2 cycles/min.
Tachigastria: The maximum electrical activity of the stomach falls in the frequency range of > 4 cycles/min.
Similar variants of the electrical activity are described for small and large intestines such as - normo-, tachy- and bradyenteria [5].
Electrical and mechanical activity is carried out by different cells synchronously, but the muscle reacts to different stimuli as a whole. There is a constant spontaneous generation of slow electric potentials in the intact gastrointestinal tract of humans and animals, which creates conditions for coordinated contractile activity of various parts of the gastrointestinal tract [6].
Slow waves of smooth muscles of various parts of mammals’ stomach and intestine are a complex of slow low-amplitude potentials, recorded on electromyograms in sawtooth (serrated) or sinusoidal waveforms, against which high-frequency potentials are reflected as spikes [3]. In other words, the wave starts with the depolarization phase. With a potential of 5-10 mV, it remains constant for some time, forming on the curve a crest of a slow wave or plateau, followed by repolarization and restoration of the membrane potential. On the crest of a slow wave, the action potential can arise (when the critical depolarization level is reached), i.e. spike [4]. The plateau phase is caused by the entrance of Ca2 + into the cell through L-type channels. Repolarization of the membrane potential can be related to inactivation of Ca2 + channels and (or) activation of K + channels (Ca2 + -dependent) [9].
Diverticular disease is characterized by changes in mucosal and muscular layers of the intestinal wall with dystrophy and atrophy of smooth myocytes. The disease occurs in less than 1% of cases, by the age of 40 it is found in 5%, in people over 80 years - in 65% of cases. And in 80% of patients diverticula are located only in the sigmoid colon, 90% - in the left part of the large intestine (including sigmoid). Localization of diverticula in the right half of the colon among residents of European countries occurs only in 4% of cases. The entire colon is rarely affected, approximately 5% of patients [4].
Diverticula are a manifestation of various pathological conditions, among which the most important are dystrophic changes in the muscular wall of the colon, discoordination of its motor skills, congenital or acquired insufficiency of the connective tissue, vascular changes in the intestinal wall. Congenital insufficiency of connective tissue is associated with a violation of collagen synthesis, which is manifested in the formation of hernial protrusions of the wall of the colon. In the appearance of diverticula in middle-aged people, an important role is played by discoordination of the motility of the colon. Against the backdrop of spasm, especially the left parts of the colon, excessive intestinal pressure leads to a divergence of muscle fibers and the formation of diverticula even in the absence of the initial degeneration of the muscular layer. Modern ideas about the development of diverticular disease also include a vascular factor: with spasm of the muscle layer, the compression of the intra-wall vessels with microcirculatory disturbance is accompanied by ischemia and retardation of venous outflow [8]. All of the above leads to dystrophic changes and expansion of circumvascular spaces, which later become the mouth of diverticula.
The mechanism of diverticulum formation is associated with a chronic process in which muscular dystrophy is observed in combination with hyperelastosis, leading to rigidity of the intestinal wall with loss of adequate response to an increase in intraluminal pressure [11]. There is also a violation of vegetative regulation of bowel function, including dysplasia of the neurons of the submucosal nerve plexus, which aggravates the disturbances in motor activity of the gut [10].
2. Materials And Methods
38 patients with diverticulosis of the colon at the age of 52 to 78 years (mean age 58.3 ± 6.2 years) were examined. In 22 patients, diverticulosis was diagnosed; in 16 patients diverticulitis was diagnosed. The comparison group consisted of 12 patients with gastro esophageal reflux disease. The electromotor activity of the stomach, ascending and descending parts of the colon was recorded with the help of surface electrodes placed in the area of the projection of the organs on the anterior abdominal wall. Evaluation of the contractile function of the colon was carried out by measuring the amplitude-frequency characteristics of the EMA.
Statistical processing of the data was carried out using the Statistica-6 software package. All quantitative data, subject to a normal distribution, are represented in the form M ± m. To process the data obtained, the Student's criterion (t) was applied with the subsequent determination of the level of reliability of the differences (p) and the χ2 criterion. Differences between the mean values were considered reliable at p < 0.05.
3. Results And Discussion
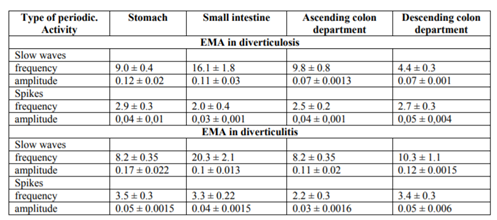
Electromotor activity of the stomach with diverticulosis in patients was characterized by the increase in the frequency of slow EMA waves by 63.6% (p < 0.05) (Table 1); EMA of the small intestine is characterized by a slight decrease in the frequency of slow waves (by 19.5%); the frequency of slow waves of the ascending colon part in diverticulosis tended to decrease (a decrease of 11%); the frequency of slow waves of the descending part of the colon at diverticulosis was practically unchanged, that is, as a whole, hypo motor dyskinesia of the large intestine was noted.
With diverticulitis, the increase in the frequency of slow waves of the small intestine was 26.3%; the frequency of slow waves and spikes in the ascending part of the colon with diverticulitis increased by 5% and 13%, respectively; the most pronounced change in the electromyogram in diverticulitis was noted in the descending section of the colon: the frequency of slow waves increased by 2.24 times, the amplitude - up to 10 times, the frequency of spikes - by 25.9%.
Thus, the electromotor activity of various parts of the digestive tract in diverticulosis is characterized by hyper motor dyskinesia of the stomach and hypo motor dyskinesia of the small and large intestine, expressed in different degrees.
With diverticulitis, hyper motor dyskinesia of the stomach, thin and descending part of the colon is observed.
4. Conclusion
It is known that a pronounced dystrophic process of ganglion neurons reduces the contractile function of smooth muscle cells of the intestinal wall. Local disturbance of blood flow with excessive development of connective tissue further disrupts the contractile function of the smooth muscle cells of the intestinal wall, which contributes to the development of stagnant phenomena in the area of the diverticulum.
EMA of the colon of patients with diverticulosis is characterized by hypo motor activity of the ascending and descending parts of the colon, which contributes to the development of constipation. Reduction of electromotor activity of the colon is an integral indicator of the neurodystrophic process, excessive collagen formation and proliferation of colon epithelium with the formation of multicellular clusters of poorly differentiated epitheliocytes.
Hyper motor dyskinesia of the stomach, small intestine and descending part of the colon, observed in diverticulitis, facilitates the acceleration of intestinal transit and the resolution of constipation..
References
- Ardatskaya M.D. Diagnostic value of the content of short chain fatty acids in irritable bowel syndrome. Rus. j gastroenterol., hepatol. And coloproctol., X (3), 36-41.(2000). Russian.
- Butov MA, Shurpo EM, Kuznetsov PS Mebeverine preparations in the treatment of functional diseases of the digestive system Experclingastroenterol5, 36-41 (2013). Russian.
- Vishnevskaya VV, Loranskaya ID, Malakhova Ye. V. Correction of motor-motor disorders of the gastroduodenal zone. Rusint journal. 2,130-133(2002). Russian.
- Vorobyev GI, Pantsirev Yu. M., Zhuchenko AP et al. Acute diverticulitis of the sigmoid colon: clinic, diagnosis, and treatment Rus. j. gastroenterol, hepatol., coloproctol. 4, 44-49 (2007). Russian.
- Zimnitskaya TV Motor dysfunction of the colon in children with chronic constipation: electrophysiological aspects Child’s health. 3, 44-47 (2015).Russian.
- Maev I. V., Gorban V. V., Nikushkina et al. Dependence of gastroduodenal blood flow on motor activity and gastric secretion in patients with peptic ulcer. Med Mess Min Intern Affairs. 2, 25-28 (2007). Russian.
- Ponomareva AP, Rachkova NS, Belmer SV, & Khavkin AI Peripheral electrogastroenteromyo -graphy in pediatric gastroenterology. (Method. aspects) - Moscow, 2007. - 48 p. Russian.
- Tat'yanchenko VK, Ovsyannikov AV, Lukash AI et al. A method for modeling diverticulosis of the large intestine. Patent RF No. 2087943 (1997). Russian.
- Ursova NI Functional disorders of the biliary tract in children as a multidisciplinary problem Almanacclinmed. 33, 47-56 (2014). Russian.
- Sheptulin AA Diverticular disease of the large intestine: clinical forms, diagnosis, treatment Rus.j. gastroenterol. hepatol. coloproctol. 5, 44-49 (2006).Russian.
- Marano L., Reda G., Porfidia R. et al. Large symptomatic gastric diverticula: two case reports and a brief review of the literature. World J Gastroenterol. 9, 36, 6114-7 (2013).