


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Hepatocellular Carcinoma in Upper Egypt: A Retrospective Study
Khairy Hammam Morsy1*, Mahmoud Saif-Al-Islam1, Esraa Maher Ibrahim2
2.Sohag Cancer center, Sohag, Egypt.
Copyright : © 2018 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Hepatocellular carcinoma (HCC) is one of the leading causes of cancer deaths worldwide. The incidence of HCC is highest in Asia and Africa, where the endemic high prevalence of hepatitis B and hepatitis C strongly predisposes to the development of chronic liver disease and subsequent development of HCC.
Aim of the Work: Our study was designed to characterize patterns of HCC cases in Sohag Governorate to lay the groundwork for future researches directed to understand the complex etiology of this disease.
Patients and Methods: The study was a retrospective one, included 215 patients with HCC over a 3 years period. Diagnosis of HCC is based on the following: criteria of HCC on triphasic computed tomography (CT) (a mass lesion with arterial enhancement and rapid washout in the porto-venous phase), serum alpha fetoprotein (AFP) level > 200 ng/mL, and/or biopsy and histopathology from the mass lesion.
Results: Evaluation of potential risk factors of HCC in cirrhotic patients revealed that patients aged ≥ 50 years had 2 times higher risk to develop HCC, while smoking increased the risk to develop HCC 4 times. Also, we found that smoking is the only factor that increased the risk (5 times higher) to develop HCC in non-cirrhotic patients, adjusted to other factors.
Conclusion: Our study showed that smoking is the most important risk factor to develop HCC in both cirrhotic and non-cirrhotic groups.
Hepatocellular carcinoma (HCC), Egypt, risk factors, cirrhosis, Gastroenterology
1. Introduction
Hepatocellular carcinoma (HCC) is a primary malignancy of the liver and occurs predominantly in patients with underlying chronic liver disease and cirrhosis. The cell(s) of origin are believed to be the hepatic stem cells, although this remains a subject of investigation[1].
HCC is one of the leading causes of cancer deaths worldwide. More than 700,000 new cases are diagnosed each year throughout the world. More than 600,000 deaths are attributed to HCC each year. The incidence of HCC is highest in Asia and Africa, where the endemic high prevalence of hepatitis B and hepatitis C strongly predisposes to the development of chronic liver disease and subsequent development of HCC[2].
The presentation of HCC has evolved significantly over the past few decades. In the past, HCC generally presented at an advanced stage with right-upper-quadrant pain, weight loss, and signs of decompensated liver disease, now it is increasingly recognized at a much earlier stage as a consequence of the routine screening of patients with known cirrhosis, using cross-sectional imaging studies and serum alpha-fetoprotein (AFP) measurements[3].
The incidence of HCC associated with hepatitis C virus (HCV) infection has not yet determined. There is also a growing problem with cirrhosis which develops in the setting of non-alcoholic fatty liver disease (NAFLD), or non-alcoholic steatohepatitis (NASH). NASH typically develops in the setting of obesity, type 2 diabetes mellitus (DM), dyslipidemia, and hypertension[4].
Resection may benefit certain patients, however many patients are not candidates given the advanced stage of their cancer at diagnosis or their degree of liver disease and, ideally, could be cured by liver transplantation. Few patients have access to transplantation, and, even in the developed world, organ shortage remains a major limiting factor. In these patients, local ablative therapies, including radiofrequency ablation (RFA), chemoembolization, and new chemotherapeutic agents, may extend life and provide palliation .
2. Aim Of The Work
Our study was designed to characterize patterns of HCC cases in Sohag Governorate to lay the groundwork for future researches directed to understand the complex etiology of this disease.
3. Patients And Methods
The study design and study population in this hospital-based case-control study was retrospectively conducted from January 2013 to January 2016 and was carried out at Sohag Cancer Center, and Department of Tropical Medicine and Gastroenterology, Sohag University Hospital, Sohag, Egypt.
The current study included 215 patients with HCC over a 3 years period. Diagnosis of HCC is based on the following: criteria of HCC on triphasic computed tomography (CT) (a mass lesion with arterial enhancement and rapid washout in the porto-venous phase), serum AFP level > 200 ng/mL, and/or biopsy and histopathology from the mass lesion.
The HCC patients were classified into the following groups:
1-Cirrhotic HCC patients (n = 190)
2-Non-cirrhotic HCC patients (n = 25)
The control groups were classified as follows:
1-Cirrhotic controls (n = 100)
2-Non-cirrhotic controls (n = 115)
Hepatocellular carcinoma in controls was ruled out by abdominal ultrasonography (US). Liver cirrhosis was diagnosed depending on suggestive history, clinical examination, laboratory, and imaging data.
For all HCC patients and controls, the following data were collected from their archive files:
1. Clinical data: age, sex, occupation, smoking, hypertension, DM, family history of malignancy, presence or absence of pallor, jaundice, lower limb edema, flapping tremor, and disturbed conscious level.
2. Laboratory investigations: complete blood count (CBC), creatinine level, complete liver function tests, prothrombin time, concentration, and international normalized ratio (INR), AFP level, and testing of hepatitis B surface antigen (HBsAg) and hepatitis C antibody (HCV Ab).
3. Imaging data: abdominal US with special stress on the number, site, and size of focal lesions, portal vein (PV) diameter, the presence or absence of PV thrombosis, ascites, and triphasic CT abdomen searching for the criteria of HCC as well as its number and size.
4. Child score, decision taken for treatment, and follow up for 6 months.
Exclusion Criteria included patients with tumors other than HCC.
4. Ethical Considerations
The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation. Data were collected by the resident doctor from the cases archive files in Sohag Cancer Center, and Department of Tropical Medicine and Gastroenterology in Sohag University Hospital. The study was approved by Ethical Committee of Faculty of Medicine, Sohag University.
5. Statistical Analysis
Data were analyzed using STATA intercooled version 12.1. Quantitative data were represented as mean, standard deviation, median and range. Data were analyzed using student t-test to compare means of two groups. When the data were not normally distributed Mann-Whitney test was used to compare two groups. Qualitative data were presented as number and percentage and compared using either Chi square test or Fisher exact test. Univariate and multivariate logistic regression analyses were used to determine the risk factors of HCC in all, cirrhotic and non-cirrhotic groups. P value was considered significant if it was less than 0.05.
6. Results
The mean ages of cirrhotic and non-cirrhotic HCC patients were 60.16 ± 9.09 and 59.76 ± 11.63 respectively. Most of the patients were more than 50 years, males, from Sohag and El-Monshah cities, and had no specific job (Table 1).
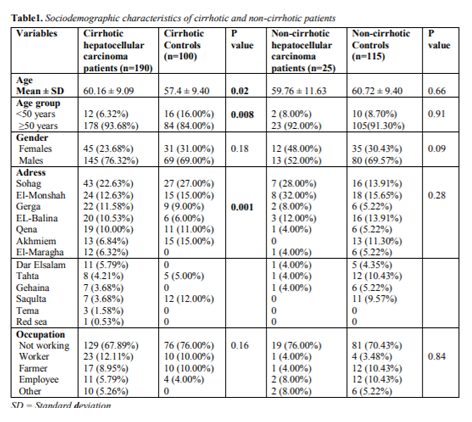
Cirrhotic HCC patients who smoke were 42.11%, while patients with hypertension and DM were 28.95% and 20.53% respectively. None has family history of HCC, while 0.53% of them had positive family history for malignancy. Jaundice was present more in cirrhotic HCC patients, while ascites, pallor, flapping tremors and lower limb edema were present more in cirrhotic controls. Cirrhotic patients with HCC had significantly higher hemoglobin level, higher platelet count, higher prothrombin concentration, lower INR, and higher serum albumin level than cirrhotic controls. Total bilirubin level was higher in cirrhotic patients with HCC than cirrhotic controls, while creatinine was normal in both groups. HCV infection and combined infection were significantly higher in cirrhotic patients with HCC than in cirrhotic controls. HBs Ag was not common in both cirrhotic HCC patients and cirrhotic controls (Table 2).
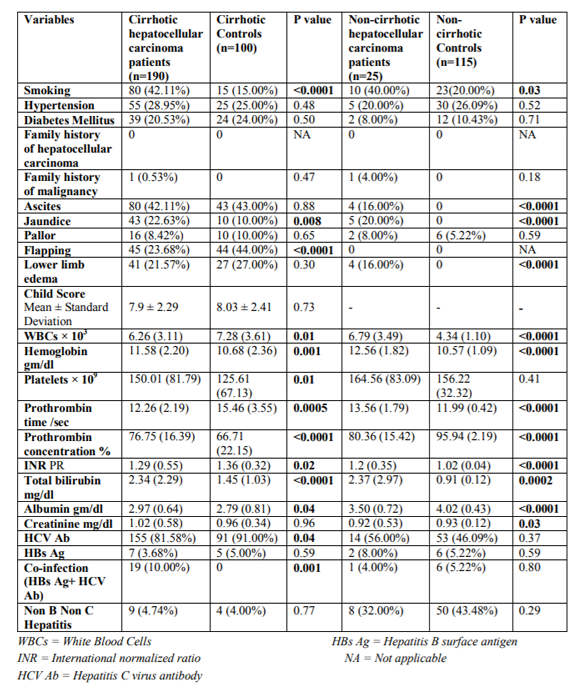
Non-cirrhotic HCC patients who smoke were 40%, while patients with hypertension and DM were 20% and 8% respectively. None has family history of HCC, while 4% of them had positive family history for malignancy. Ascites was present in 16%, jaundice in 20%, pallor in 8%, and lower limb edema in 16%. Non-cirrhotic HCC patients showed significantly higher hemoglobin level, lower prothrombin concentration, higher INR, higher total bilirubin level, and lower serum albumin level than non-cirrhotic controls. Creatinine was normal in both groups. HCV Ab was present more in non-cirrhotic HCC patients than non-cirrhotic controls without statistical significance. HBsAg is not common in both non-cirrhotic HCC patients and non-cirrhotic controls (Table 2).
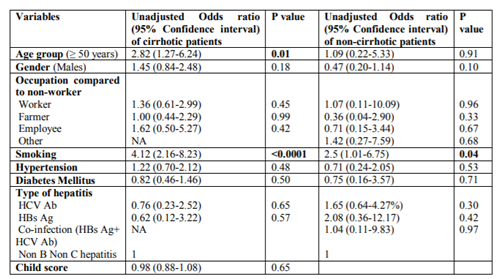
Univariate analysis of potential risk factors of HCC in cirrhotic patients revealed that age ≥ 50 years and smoking had significant higher risk to develop HCC. In non-cirrhotic patients smoking was associated with a significant higher risk to develop HCC (Table 3).
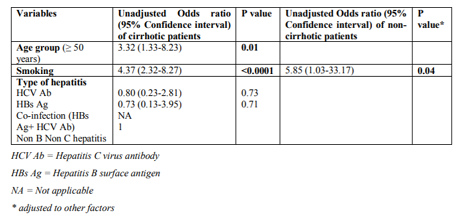
Multivariate analysis of potential risk factors of HCC in cirrhotic patients revealed that patients aged ≥ 50 years had 2 times higher risk to develop HCC, while smoking increased the risk to develop HCC 4 times. In non-cirrhotic patients smoking is the only factor that increased the risk (5 times higher) to develop HCC, adjusted to other factors (Table 4).
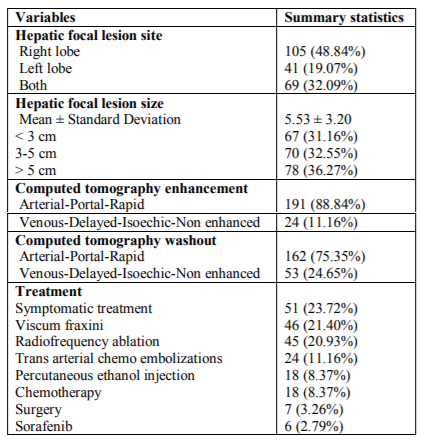
From our study we found that HCC was commonly found in right lobe (48.84%), followed by both lobes (32.09%), and lastly left lobe (19.07%). The hepatic focal lesions ranged from 1-16 cm with a mean of 5.53 ± 3.20 cm. Most of the patients (88.84%) had the typical criteria of triphasic CT enhancement, and 75.35% had typical wash out criteria. 23.72% of patients were given symptomatic treatment, followed by viscum fraxini (21.40%), then radiofrequency ablation (20.93%) (Table 5).
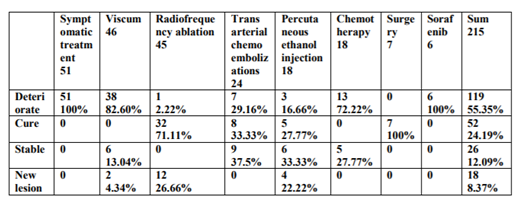
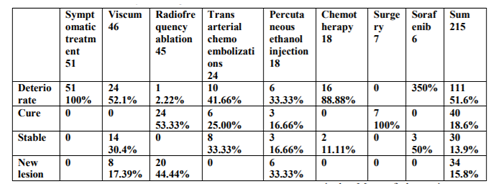
Some treatment options had no cure rate after 3 months or 6 months like symptomatic treatment, viscum fraxini, chemotherapy, and sorafenib. Transarterial chemembolizations, and percutaneous ethanol injection had high cure rates of 33.33%, 27.77% after 3 months and 25 %, 16.66% after 6 months respectively. Radio frequency ablation and hepatic resection had the best cure rates; 71.11%, 100% after 3 months and 53.33%, 100% after 6 months respectively (Tables 6,7). Survival rate after 3 and 6 months follow up was 100% in all methods of treatment.
7. Discussion
Hepatocellular carcinoma represents 85%-90% of primary liver cancers accounting for 3.5% and 7.5% of all cancers among women and men respectively, and accounts for half a million deaths per year. It is rarely detected early and usually fatal within few months of diagnosis[5]. The incidence of HCC is increasing, and currently it is the second leading cause of cancer-related death worldwide, accounting for approximately 800000 deaths every year[6]. In Egypt, the incidence of HCC has been nearly doubled over the last decade[7].
In our study the mean ages of cirrhotic and non-cirrhotic HCC patients were 60.16 and 59.76 years respectively. Most of the patients were males more than 50 years old. Age of 50 years or more was considered a significant risk factor to develop HCC. This is in agreement with Soliman et al.[8] who reported that the mean age of HCC patients was 56.02 years, 84% of them were males, and 16% were females. Also, Zaky et al.[9] found the mean age of HCC was 58.61 years and more than 80% of the patients were males. Most of HCC patients were from Sohag and El-Monshah cities. This could be due to the high population density in these areas.
We found that smoking was significantly higher in cirrhotic and non cirrhotic HCC patients than in the control. This is in agreement with Morsy et al.[10] who found that tobacco smoking was a risk factor of HCC in both cirrhotic and non-cirrhotic patients. Mizoue et al.[11] observed a three times higher risk of HCC among smokers compared to nonsmokers. Additionally, another study found a 50% increase in risk of HCC for current male smokers compared to nonsmokers[12]. In contrast, Zhu et al.[13] did not observe a significantly increased risk of HCC among current male smokers after conducting a population based, case control study. Male x-smokers had a significant increase in risk of HCC suggesting a dose or duration response underlying this association. In addition to increase in risk of developing HCC, a cohort study suggested that smoking increases risk of death from HCC[14].
In our study arterial hypertension was insignificantly higher in cirrhotic patient with HCC than in cirrhotic controls. Arterial hypertension has been described as a paraneoplastic manifestation of HCC. Some cases of severe arterial hypertension associated with high plasma level of angiotensin-I, accompanied with hypokalemia have been reported[15]. Elevated concentrations of angiotensinogen have been found, whether or not associated with higher plasma levels of renin. Overproduction of angiotensinogen and renin could both play a role in causing paraneoplastic hypertension in patients affected by HCC[16].
Diabetes Mellitus was not considered a significant risk factor for HCC in our study. About 20% of cirrhotic group in our study were diabetic that was nearly similar to the prevalence of DM among HCC patients in Abdel-Wahab et al.[17] study which was 13.6%. An Egyptian study revealed high prevalence of DM in liver cirrhosis and HCC but no statistically significant difference in prevalence of DM between HCC and liver cirrhosis patients[18]. In contrast, Lagiou et al.[19] found a positive correlation between the history of DM and HCC.
Family history of HCC was not found in our study, although significant association was observed between family history of HCC and primary liver cancer in a study conducted by Fernandez et al.[20]. Also, Turati et al.[21] found that patients with a positive family history of liver cancer have a 2- to 3-fold increase in their HCC risk. This may be due to the relatively small number of our study population. Positive family history of malignancy was 8.05% (not significant) according to Soliman et al., while in our study it was 0.53%, 4% in the cirrhotic and non-cirrhotic HCC patients respectively.
Cirrhotic patients with HCC had significantly higher hemoglobin level, higher platelet count, shorter prothrombin time, higher prothrombin concentration, lower INR, and higher serum albumin level than cirrhotic controls. This is because the controls were hospitalized patients in late stage of cirrhosis. This explains also why flapping tremor was significantly more present among cirrhotic controls.
Erythrocytosis complicating HCC results from the synthesis and secretion by the tumor of erythropoietin in native or slightly altered form[22,23]. Patients with HCC sometimes have erythrocytosis and high plasma erythropoietin levels[24]. Production of biologically active erythropoietin by malignant hepatocytes is not unexepected because this hormone is normally synthesized by the fetal liver[25].
Total bilirubin level was higher in cirrhotic patients with HCC than cirrhotic controls. This can be explained by Carr et al.[26] who found association between abnormal bilirubin and aggressive HCC even in patients with small size tumors, which could not cause liver failure.
As expected non-cirrhotic HCC patients showed significantly prolonged prothrombin time, lower prothrombin concentration, higher INR, higher total bilirubin level, and lower serum albumin level than non-cirrhotic controls.
Majority of HCC patients were cirrhotic as a result of viral infection. Most of patients (81.58%) had positive HCV Ab followed by co-infection (HBs Ag+ HCV Ab) (10%), then non B non C hepatitis (4.74%), and lastly positive HBsAg (3.68%). These results were similar to Abdel-Wahab et al. who found that hepatitis C, B and co-infection were76.6%, 3.3%, and 3.6% respectively.
The etiology of liver cirrhosis and HCC in Zaky et al.9 study was HCV infection in approximately 56.8% of the patients, hepatitis B virus (HBV) infection in approximately 2.7% of the patients, and combined HCV & HBV infection in approximately 2.7% of the patients. The prevalence of HCV in their study (56.8%) was lower than that in our study (81.58%) because in their study hepatitis markers were not performed in 37.8% of patients.
The independent effect of hepatitis viruses in the etiology of HCC had been recognized and confirmed in Yates et al.[27]and El-Zayadi et al.[28]studies. There is a strong association between cirrhosis and HCC[29].
Several small-scale hospital-based studies have been conducted to examine the etiologic significance of the primary HCC risk factors in Egypt[30]. These studies have shown the increasing importance of HCV in liver cancer, accounting for 40-50% of liver cancer cases, and the declining influence of HBV and HBV/HCV infection, accounting for 25% and 15%, respectively[31]. The WHO has reported HBV to be second only to tobacco as a known human carcinogen[32]. Although HBV is considered worldwide as a major risk factor for liver cirrhosis and HCC, the prevalence of HBV infection in Egypt has been declining over the last two decades[33].
Our results revealed that, the percentage of right, left, and both lobes HCC were 48.84%, 19.07%, and 32.09% respectively. However, Abdel-Wahab et al. reported that the right lobe was the site for HCC lesions in 63.9%, left lobe in 25.8% and both lobes in 10.3% of the patients.
In our study tumor size >5 cm was detected in 36.27% of patients and this is much lower than what was reported in Abdel-Wahab et al. study in which 65.5% of patients had tumor size >5 cm. This may be due to the increased awareness of the patients about liver diseases and sonographic screening programs of HCC in most of the hospitals.
The type of treatment given to HCC patients in our study was symptomatic treatment in 23.72%, viscum fraxini in 21.40 %, radiofrequency ablation in 20.93%, transarterial chemo embolizations in 11.16%, percutaneous ethanol injection in 8.37 %, chemotherapy in 8.37%, hepatic resection in 3.26%, and sorafenib in 2.79%. Our results were different from those of Zaky et al. where transarterial chemo embolizations was done in 32.4%, local ablation therapy in 29.7%, palliative therapy in 28.4%, and hepatic resection in 9.5%. Also, our results were different from those of Abdel-Wahab et al. who reported that 38.7% were managed by conservative treatment, hepatic resection in 25.8%, chemoembolizations in 17.2%, radiofrequency in 13.1%, mixed treatment in 3.5%, while alcohol injection was done in 0.9% of patients. The cause of the above mentioned differences can be explained by many reasons like the time of presentation, availability or not of some methods like transarterial chemoembolizations and radiofrequency ablation needles, consultants and specialists, availability of drugs like viscum fraxini, chemotherapy, and others, and according to strategy of Sohag Cancer Institute, or different culture as some patients in our study were eligible for resection but they asked for another modality and were shifted to local ablation therapy, as well as some patients were not fit for surgery.
Radiofrequency ablation and hepatic resection had the best cure rates this is in agreement with many other studies34-36. The 5-year survival rates after resection can exceed 50 %. Ablation had survival rates comparable to resection[37].
References
- Alison MR: Liver stem cells: implications for hepatocarcinogenesis. Stem Cell Rev; 1(3): 253-60 (2005).
- Dhanasekarar R, Limaye A, Cabrera R: Hepatocellular carcinoma: current trends in worldwide epidemiology, risk factors, diagnosis, and therapeutics. Hepat Med; 4: 19-37 (2012).
- Llovet JM, Fuster J, Bruix J: The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl; (2 Suppl 1): S115-20.
- Bugianesi E (2007): Non-alcoholic steatohepatitis and cancer. Clin Liver Dis; (1): 191-207 (2004).
- Hamed MA, Ali SA: Non-viral factors contributing to hepatocellular carcinoma. World J Hepatol; 5(6): 311-22 (2013).
- Gomaa AI, Waked I: Recent advances in multidisciplinary management of hepatocellular carcinoma. World J Hepatol; 7(4): 673-87 (2015).
- Abu El Makarem M: Overview of Biomarkers for the Diagnosis of Hepatocellular Carcinoma. Hepat Mon; 12(10 HCC): e6122 (2012).
- Soliman AS, Hung C, Tsodikov A, Seifeldin IA, Ramadan M, Al-Gamal D, Schiefelbein EL, Thummalapally P, Dey S, Ismail K: Epidemiologic risk factors of hepatocellular carcinoma in a rural region of Egypt. Hepatol Int; 4: 681-90 (2010).
- Zaky S, Makhlouf NA, Abdel-Malek MO, Bakheet AA, Seif HM, Hamza HM, Sabry AM: Multidisciplinary decision making in the management of hepatocellular carcinoma: A hospital-based study. Turk J Gastroenterol; 26: 498-505 (2015).
- Morsy KH, Hasanain AF, Kobeisy MA: Risk factors of hepatocellular carcinoma: are they the same among cirrhotic and noncirrhotic patients in upper Egypt? J Arab Soc Med Res; 6:103-10 (2011).
- Mizoue T, Tokui N, Nishisaka K, Nishisaka S, Ogimoto I, Ikeda M, Yoshimura T: Prospective study on the relation of cigarette smoking with cancer of the liver and stomach in an endemic region. International Journal of Epidemiology; 29: 232-7 (2000).
- Yun YH, Jung KW, Bae JM, Lee JS, Shin SA, Min Park S, Yoo T, Yul Huh B: Cigarette smoking and cancer incidence risk in adult men: National Health Insurance Corporation Study. Cancer Detect Prev; 29:15-24 (2005).
- Zhu K, Moriarty C, Caplan LS, Levine RS: Cigarette smoking and primary liver cancer: a population-based case-control study in US men. Cancer Causes Control; 18:315-21 (2007).
- Jee SH, Ohrr H, Sull JW, Samet JM: Cigarette smoking, alcohol drinking, hepatitis B, and risk for hepatocellular carcinoma in Korea. Journal of the National Cancer Institute; 96: 1851-6 (2004).
- Arai H, Saitoh S, Matsumoto T, Makita F, Mitsugi S, Yuasa K, Takagi H, Mori M: Hypertension as a paraneoplastic syndrome in hepatocellular carcinoma. Journal of gastroenterology; 34(4): 530-4 (1999).
- Kew MC, Leckie BJ, Greeff MC: Arterial hypertension as a paraneoplastic phenomenon in hepatocellular carcinoma. Arch Intern Med; 149: 2111-3 (1989).
- Abdel-Wahab M, El-Ghawalby N, Mostafa M, Sultan A, El-Sadany M, Fathy O, Salah T, Ezzat F: Epidemiology of hepatocellular carcinoma in lower Egypt, Mansoura Gastroenterology Center. Hepatogastroenterology; 54: 157-62 (2007).
- Bakir AS, Ali-Eldin ZA: Is diabetes mellitus a risk factor for hepatocellular carcinoma in Egyptian patients? J Am Sci; 8: 353-8 (2012).
- Lagiou P, Kuper H, Stuver SO, Tzonou A, Trichopoulos D, Adami H: Role of diabetes mellitus in the etiology of hepatocellular carcinoma. J Natl Cancer Inst; 92: 1096-9 (2000).
- Fernandez E, La Vecchia C, D'Avanzo B, Negri E, Franceschi S: Family history and the risk of liver, gallbladder, and pancreatic cancer. American Association for Cancer Research; 3: 209-12 (1994).
- Turati F, Edefonti V, Talamini R, Ferraroni M, Malvezzi M, Bravi F, Franceschi S, Montella M, Polesel J, Zucchetto A, La Vecchia C, Negri E, Decarli A: Family history of liver cancer and hepatocellular carcinoma. Hepatology; 55: 1416-25 (2012).
- Kew MC, Fisher JW: Serum erythropoietin concentrations in patients with hepatocellular carcinoma. Cancer; 58(11): 2485-8 (1986).
- Matsuyama M, Yamazaki O, Horii K, Higaki I, Kawai S, Mikami S, Higashino M, Oka H, Nakai T, Inoue T: Erythrocytosis caused by an erythropoietin-producing hepatocellular carcinoma. J Surg Oncol; 75(3): 197-202 (2000).
- Sakisaka S, Watanabe M, Tateishi H, Harada M, Shakado S, Mimura Y, Gondo K, Yoshitake M, Noguchi K, Hino T, Nohno R, Majima Y, Hirai K, Sata M, Yoshida H, Tanikawa K: Erythropoietin production in hepatocellular carcinoma cells associated with polycythemia: immunohistochemical evidence. Hepatology; 18 (6): 1357-62 (1993).
- Mirand EA, Zucali JR, Murphy GP: Role of liver in erythropoietin production: clinical and experimental evidences. N Y State J Med; 76(7): 1100-2 (1976).
- Carr IB, Guerra V, Giannini EG, Farinati F, Ciccarese F, Rapaccini GL, Marco MD, Benvegnù L, Zoli M, Borzio F, Caturelli E, Chiaramonte M, Trevisani F: Association of abnormal plasma bilirubin with aggressive HCC phenotype. Semin Oncol; 41(2): 252-8 (2014).
- Yates SC, Hafez M, Beld M, Lukashov VV, Hassan Z, Carboni G, Khaled H, McMorrow M, Attia M, Goudsmit J: Hepatocellular carcinoma in Egyptians with and without a history of hepatitis B virus infection: association with hepatitis C virus (HCV) infection but not with HCV RNA level. Am J Trop Med Hyg; 60: 714-20 (1999).
- El-Zayadi AR, Badran HM, Barakat EM, Attia Mel-D, Shawky S, Mohamed MK, Selim O, Saeid A: Hepatocellular carcinoma in Egypt: a single center study over a decade. World J Gastroenterol; 11: 5193-8 (2005).
- Darwish MA, Faris R, Darwish N, Shouman A, Gadallah M, El-Sharkawy MS, Edelman R, Grumbach K, Rao MR, Clemens JD: Hepatitis C and cirrhotic liver disease in the Nile Delta of Egypt: a community-based study. Am J Trop Med Hyg; 64: 147-53(2001).
- Lehman EM, Soliman AS, Ismail K, Hablas A, Seifeldin IA, Ramadan M, El-Hamzawy H, Shoushtari CS, Wilson ML: Patterns of hepatocellular carcinoma incidence in Egypt from a population-based cancer registry. Hepatol Res; 38(5): 465-73 (2008).
- Strickland GT, Elhefni H, Salman T, Waked I, Abdel-Hamid M, Mikhail NN, Esmat G, Fix A: Role of hepatitis C infection in chronic liver disease in Egypt. Am J Trop Med Hyg; 67: 436-42 (2002).
- WHO: Department of Communable Diseases, Surveillance and Response: WHO. Hepatitis B (2002).
- Khattab MA, Eslam M, Sharwae MA, Hamdy L: Seroprevalence of hepatitis C and B among blood donors in Egypt: Minya Governorate, 2000-2008. Am J Infect Control; 38:640-1 (2010).
- Kim KH, Choi YK: Long-term survival after resection of hepatocellular carcinoma. Korean J Hepatobiliary Pancreatic Surg; 16(3): 98-104 (2012).
- Shaya FT, Breunig IM, Seal BCD, Chirikov VMullins VV, Hanna N: Comparative and Cost Effectiveness of Treatment Modalities for Hepatocellular Carcinoma in SEER-Medicare. PharmacoEconomics; 32: 63 (2014).
- Changyong E, Wang D, Yu Y, Liu H, Ren H, Jiang T (2017): Comparison of radiofrequency ablation and hepatic resection for hepatocellular carcinoma: A meta-analysis. J Can Res Ther; 13: 625-30.
- Bruix J, Sherman M: Management of hepatocellular carcinoma: an update. Hepatology; 53:1020-2 (2011).