


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
The Impact of Gender on the Symptom Presentation and Life Quality of Patients with Erosive Esophagitis and Non-Erosive Reflux Disease
Shou-Wu Lee 1,2, Teng-Yu Lee 1,2, Han-Chung Lien 1,3, Sheng-Shun Yang 1,3, Hong-Zen Yeh 1,3, Chi-Sen Chang1,2
2 Department of Internal Medicine, Chung Shan Medical University, Taichung, Taiwan
3 Department of Internal Medicine, National Yang-Ming University School of Medicine, Taipei, Taiwan
Copyright : © 2016 Shou-Wu L. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background/purpose: Gastroesophageal reflux disease (GERD) can be classified as erosive esophagitis (EE) or non-erosive reflux disorder (NERD) by endoscopic findings. The aim of this study was to investigate the effect of gender on symptom presentation and quality of life of patients with EE and NERD.
Methods: Data from patients with GERD were collected between January and December 2009. The enrolled patients were assigned either to the EE or to the NERD group. The general demographic data, the modified Chinese GERDQ scores and the SF-36 life quality questionnaire scores of the three groups of patients were compared.
Results: Among the 261 enrolled patients, 87, 86 and 88 patients were classified into the EE, NERD and control groups, respectively. The EE group patients were significantly older, predominately male, had more hiatal hernia, higher body weight and BMI, than those in the NERD group. GERD-specific symptom scores and general life quality scores of the EE and NERD groups were similar, and both groups had lower life quality scores than the control group did. The female patients with NERD had a higher frequency of GERD symptoms and lower quality of life scores. Gender had no effect on symptom scores or life quality scores in the EE group.
Conclusion: The GERD-specific symptom severity and general quality of life scores of the EE and NERD patients were similar. Gender had a great influence on symptom presentation and life quality of patients with NERD, but not of those with EE.
Keywords: Erosive Esophagitis; Gastroesophageal Reflux Disease; Gender; Life Quality; Non-Erosive Reflux Disease
Abbreviations:
EE: Erosive Esophagitis; NERD: Non-Erosive Reflux Disease
1.Introduction
Gastroesophageal reflux disease (GERD) is a chronic disease that tends to relapse and cause complications. According to the Montreal definition, GERD is ‘a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications’[1]. The cardinal symptoms of GERD are considered to be heartburn and regurgitation. Besides, GERD is also associated with a range of other symptoms originating in the esophagus, chest and respiratory tract [2]. Based on the presence or absence of mucosal damage, GERD patients can be classified as having either erosive esophagitis (EE) or non-erosive reflux disorder (NERD) [3]. GERD has an impact on the daily lives of affected individuals, interfering with physical activity, impairing social functioning, disturbing sleep and reducing productivity at work [4,5]. The aim of this study was to investigate the impact of gender on the symptom presentation and quality of life among patients with EE and NERD.
2.Methods
Data from 261 consecutive patients diagnosed with GERD in our hospital, according to the Montreal definition, were collected between January 2009 and December 2009. Exclusion criteria were as follows: (1) GERD combined with other structural gastrointestinal disorders, such as peptic ulcer disease, esophageal or gastric malignancy, (2) prior gastric surgery, (3) use of chronic anti-acid medication, such as proton pump inhibitors (PPIs) or H2-receptor antagonists (H2RAs), for more than 2 months prior to enrollment, and (4) pregnancy.
The general data of enrolled patients, including age, gender, body weight, body mass index (BMI), symptom duration and lifestyle habits, were recorded. All patients underwent an open-access transoral upper gastrointestinal endoscopy, and the findings of each case were collected.
These patients were assigned to two groups according to whether they had esophagocardiac mucosal break (EE group) or not (NERD group) detected by upper gastroinestinal endoscopy. All patients were asked to complete two questionnaires, the modified Chinese GERDQ and the SF-36 questionnaire (Chinese version). Patients without typical symptoms of GERD and normal endoscopic findings during this period were assigned to the control group. The general data and questionnaire scores were analyzed.
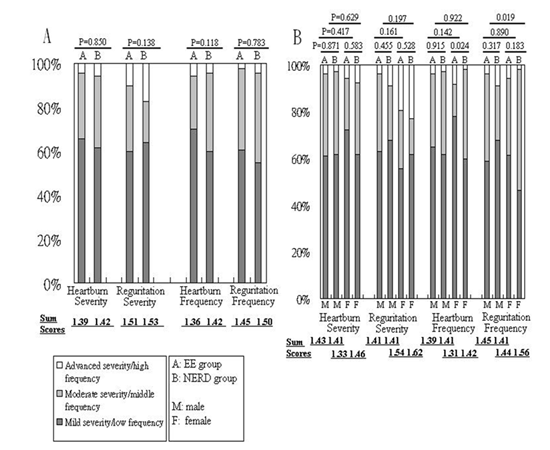
The modified Chinese GERDQ includes questions about the severity and frequency of the symptoms of regurgitation and heartburn, and answers are graded on a three-point Likert scale. Mild, moderate and advanced severity were defined as symptoms that can be easily ignored, awareness of symptoms but easily tolerated, and symptoms sufficient to cause an interference with normal activities, respectively. Low, middle, and high frequency symptoms were classified as those occurring at least once per month, at least once a week, and at least once a day, respectively.
The SF-36 questionnaire measures general quality of life, which allows comparisons between different disease states. It measures health status in eight domains: physical functioning, role limitations-physical, bodily pain, general health, vitality, social functioning, role limitations-emotional, and mental health. Two summary scores are also calculated from subject responses: the physical health (PH) score and the mental health (MH) score. Scores on the SF-36 range from 0 to 100 on each dimension and on the summary scales, with higher scores indicating better quality of life.
Data are expressed as standard derivation of mean for each of the measured parameters. Gender, hiatal hernia, lifestyle habits and the modified Chinese GERDQ items, are expressed as a percentage of the total patient number. A p value below 0.05 was considered statistically significant. Statistical analyses were made using Pearson’s chi-square test or Fisher’s exact test to compare the effects of gender on hiatal hernia, lifestyle habits and the modified Chinese GERDQ scores; ANOVA was used to analyze the effects of age, symptom duration, body weight, BMI, and scores of SF36 questionnaires.
3.Results
A total of 261 consecutive patients were enrolled, with 87, 86, and 88 patients assigned to the EE group, the NERD group, and the control group, respectively. As shown in Table 1, the EE group patients were significantly older (mean 48.94 years old vs. 43.34 years old), predominately male (58.6% vs. 39.5%), had hiatal hernia (34.5% vs 17.4%), higher body weight (67.57 kg vs. 61.06 kg) and BMI (24.09kg/m2 vs. 22.68 kg/m2) than patients in the NERD group. The two groups had similar GERD symptoms and lifestyle habits, including tea, alcohol, coffee consumption and cigarette smoking.
As displayed in Figure 1A, the rates of severity and frequency of heartburn and acid regurgitation, as measured by the modified Chinese GERDQ, were similar between the two groups, although the patients in the NERD group had the relatively higher scores in all items.
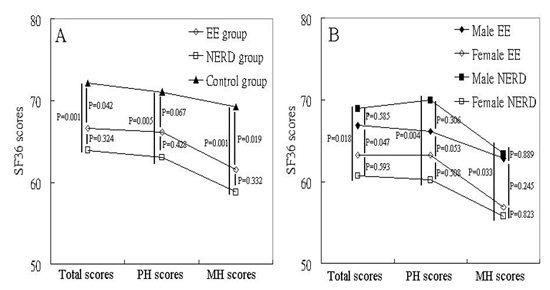
The total scores, PH scores and MH scores, as measured by the SF-36 questionnaire are shown in Figure 2. The patients in the NERD group had the lowest scores (mean total score 63.93, PH score 64.03, MH score 58.80), followed by those in the EE group (mean total score 66.61, PH score 66.13, MH score 61.53) and those in the control group (mean total score 72.16, PH score 71.02, MH score 69.27). There were no significant differences between the EE group and the NERD group.
The impacts of gender on the symptom presentation are displayed in Figure 1B. The severity and frequency of regurgitation were significantly greater in the female NERD patients than in the male NERD patients (P=0.019). There was no difference in the presentations of heartburn or regurgitation between men and woman in the EE group. In general, the female NERD patients had the worst scores of the severity and frequency in both symptoms.
The scores of the SF-36 questionnaire are summarized in Figure 2B. The scores of the men and women in the EE group were similar, but significantly lower scores were noted in the female NERD patients (mean total score 60.67, PH score 60.19, MH score 55.81) than in the male NERD patients (mean total score 78.91, PH score 69.91, MH score 63.38). Additionally, compared to the control cases, only the female patients in the NERD group had significantly lower scores in both the physical (P=0.002) and mental (P=0.005) dimensions.
EE: erosive esophagitis; NERD: non-erosive reflux disease.
EE: erosive esophagitis; NERD: non-erosive reflux disease; SF-36: Short-form 36; PH: Physical health; MH: Mental health.
5.Discussion
GERD is very common in the general population, and it has a considerable impact on the daily lives of affected individuals. The two subtypes of this disease, NERD and EE, have different presentations and impacts on the quality of life of each patient. NERD may account for 60% of all chronic heartburn cases in a community. It is now well established that NERD is associated with impaired quality of life, which is at the very least as severe as that related to erosive disease and complicated GERD [6, 7].
A study that enrolled 153 patients showed that the EE group had higher BMI levels, and a higher proportion of male subjects, current smokers and alcohol consumers, compared to the NERD and control group [8]. Another population-based study disclosed that male gender, overweight, regular use of alcohol, a longer history of GERD and smoking were independent predictors of EE. However, no single factor was capable of predicting mucosal damage with clinically sufficient certainty [9]. In addition, men and subjects with hiatal hernia had a higher risk of EE according to the results of one study [10]. In multivariate analysis, old age, male gender, moderate working burden, divorced, widowed status and strong tea drinking remained as significant independent risk factors for EE [11].
Our results proved there were strong positive correlations of older age, male-predominance, lower body weight and BMI, and a higher proportion of hiatal hernia in patients with EE, compared to those with NERD. However, in our study, the lifestyle habits and symptom duration between the two groups were similar, which might be due to the limited number of enrolled cases, or the different pathogenesis of EE in the Chinese population.
Previous studies indicated there were no significant differences between EE and NERD patients in any of the symptom severity scores [12-14]. A meta-analysis of five trials incorporating a total of 11,945 GERD subjects found no correlation between the severity of esophagitis and symptoms [15]. In our study, the severity and frequency of heartburn or regurgitation were similar in the EE and NERD groups. However, the female patients in the NERD group had the worst symptom presentation, especially in the dimension of regurgitation, which was compatible with the result of a previous study [12].
Patients with GERD may present with a broad range of troublesome symptoms that can adversely affect the quality of daily life. A German study determined that patients with GERD were substantially impaired, both physically and psychosocially, compared with the general population [14]. A Chinese study reported that the largest impairments in subjects with GERD symptoms were related to bodily pain and role limitations among all subscales [16]. Another study documented patients with GERD as impaired in pain but less impaired in physical and role functioning dimensions [17]. Other studies reported the EE and NERD cases had similar total quality of life scores [8, 13, 14].
In our study, patients with EE and those with NERD had similar general quality of life scores. However, compared with the normal population, the NERD patients had significantly impaired quality of life in most dimensions, but the EE patients didn’t. The results implied that GERD might have a more negative impact on the NERD patients than on the EE cases.
Taking into consideration the impact of gender on quality of life in patients with GERD, a previous study found women in the EE group had worse general scores [12]. Our study had conflicting findings showing that women had significantly lower scores compared to men in the NERD group, but not in the EE group. The trends might be due to a heightened sensitivity and symptom perception of female patients with NERD.
There were some limitations in our study. Firstly, the endoscopic findings were recorded by individual endoscopists, and inter-observer conflict and misclassification might have occurred. Secondly, co-morbid diseases of these patients that tend to influence severity of GERD, such as chronic heart failure or chronic obstructive pulmonary disease, were not considered, and this might have led to inaccurate outcomes. Thirdly, the lifestyle characteristics in our study were only limited to the patients’ current status. Lastly, our study was hospital-based. Further research using representative samples of the general population are needed to confirm these results.
5.Conclusion
In the present study, patients with EE were older, predominately male, had more hiatal hernia, higher body weight and BMI, than those with NERD. The two groups had similar GERD-specific symptom severity and general quality of life scores. Gender had a great influence on symptom presentation and life quality of patients with NERD, but less impact on those with EE.
References
- Vakil N, Veldhuyzen van Zanten S, Kahrilas P, Dent J and Jones R. The Montreal definition and classification of gastro-esophageal reflux disease (GERD) – a global evidence-based consensus. Am J Gastroenterol 101:1900–1920 (2006)
- Ronkainen J, Aro P, Storskrubb T, Lind T, Bolling-Sternevald E, Junghard O, Talley NJ and Agreus L. Gastroesophageal reflux symptoms and health related quality of life in the adult general population — the Kalixandra study. Aliment Pharmacol Ther. ;23:1725–1733 (2006)
- Armstrong D, Bennett JR, Blum A, Dent J, De Dombal FT, Galmiche JP, Lundell L, Margulies M, Richter JE, Spechler SJ, Tytgat GN and Wallin L. The endoscopic assessment of esophagitis: a progress report on observer agreement. Gastroenterology 111:85–92 (1996)
- Wiklund I. Review of the quality of life and burden of illness in gastroesophageal reflux disease. Dig Dis 22:108–114 (2004)
- Wahlqvist P, Karlsson M, Johnson D, Carlsson J, Bolge SC and Wallander MA. Relationship between symptom load of gastro-oesophageal reflux disease and health-related quality of life, work productivity, resource utilization and concomitant diseases: survey of a US cohort. Aliment Pharmacol Ther. 27(10):960–970 (2008)
- Fass R, Fennerty MB and Vakil N. Non-erosive reflux disease (NERD)—current concepts and dilemmas, Am J Gastroenterol. 96:303–314 (2001)
- Quigley EM. Non-erosive reflux disease: part of the spectrum of gastrooesophageal reflux disease, a component of functional dyspepsia, or both?, Eur J Gastroenterol Hepatol, 13 (Suppl 1):S13–18. (2001)
- Oh JH, Kim TS, Choi MG, Lee H, Jeon EJ, Choi SW, Lee C and Chung IS. Relationship between psychological factors and quality of life in subtypes of gastroesophageal reflux disease. Gut Liver. 3(4):259–265 (2009)
- Labenz J, Jaspersen D, Kulig M, Leodolter A, Lind T, Meyer-Sabellek W, Stolte M, Vieth M, Willich S and Malfertheiner P. Risk factors for erosive esophagitis: a multivariate analysis based on the ProGERD study initiative. Am J Gastroenterol. 299:1652–1656 (2004)
- Ronkainen J, Aro P, Storskrubb T, Johansson SE, Lind T, Bolling-Sternevald E, Graffner H, Vieth M, Stolte M, Engstrand L, Talley NJ and Agreus L. High prevalence of gastroesophageal reflux symptoms and esophagitis with or without symptoms in the general adult Swedish population: a Kalixanda study report. Scand J Gastroenterol. 40(3):275–285 (2005)
- Du J, Liu J, Zhang H, Yu CH and Li YM. Risk factors for gastroesophageal reflux disease, reflux esophagitis and non-erosive reflux disease among Chinese patients undergoing upper gastrointestinal endoscopic examination. World J Gastroenterol. 13(45):6009–6015 (2007)
- Lippmann QK, Crockett SD, Dellon ES and Shaheen NJ. Quality of life in GERD and Barrett's esophagus is related to gender and manifestation of disease. Am J Gastroenterol. 104(11):2695–2703 (2009)
- Kovacs Z and Kerekgyarto O. Psychological factors, quality of life, and gastrointestinal symptoms in patients with erosive and non-erosive reflux disorder. Int J Psychiatry Med. 37(2):139–150 (2007)
- Kulig M, Leodolter A, Vieth M, Schulte E, Jaspersen D, Labenz J, Lind T, Meyer-Sabellek W, Malfertheiner P, Stolte M and Willich SN. Quality of life in relation to symptoms in patients with gastro-oesophageal reflux disease—an analysis based on the ProGERD initiative, Aliment Pharmacol Ther. 18:767–776 (2003)
- Fennerty MB and Johnson DA, Heartburn severity does not predict disease severity in patients with erosive esophagitis, Med Gen Med. 8:6 (2006)
- Chen M, Xiong L, Chen H, Xu A, He L and Hu P. Prevalence, risk factors and impact of gastroesophageal reflux disease symptoms: A population-based study in South China. Scand J Gastroenterol. 240:759–767 (2005)
- Revicki DA, Wood M, Maton PN and Sorensen S. The impact of gastroesophageal reflux disease on health-related quality of life. Am J Med. 104:252–258 (1998)