


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Violent Death among Adult Egyptian Women from Cairo and Giza during 2011-2012
Nadia A. Kotb1*, Samah Ebrahim1
Copyright :© 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Violence against women is a well-recognized form of human women violation, and death is the most severe consequence of violence. This study aims at evaluation of the pattern of deadly violence in our community. A retrograde study including 317 adult women from the 3rd to 9th decades of age, was conducted on women autopsied at Zeinhom mortuary during 2011 and 2012, who were drained from Cairo and Giza Governorates. Statistical analysis of the obtained results, showed that the victimized women from Cairo were more than from Giza (61.2%) (38.8%). The majority were at the 3rd decade of life (45%) mostly married (44.5%), and the scene of death was mostly at home (57.7%), at day time (a.m.) 23.7%, during summer months (4th, 5th) or autumn (9th, 10th). Homicidal Femicides were more than half the cases (50.2%), followed by accidental deaths (24.6%), then suicides (9.1%). Associated poisoning were detected in (6%) of the study cases. Injuries by sharp and blunt weapons contributed to (49.2%) of homicidal deaths and violent asphyxias to (27.3%) of them, but fire – arm injuries were mostly accidental (20.5%) rather than homicidal (18.7%). The assailant was undetermined at time of autopsy in (36.6%) of cases, and the husband was the suspected assailant in (23.8%) of homicidal deaths.
Keywords: Violent Death, Adult Egyptian Women,Cairo,Giza,Forensic Science
1.Introduction
Violence is a world - wide socio demographic problem. The report of WHO (1996) on global violence focused on violence as a major health priority. About one million individuals lose their lives each year due to violence (Krug, et al, 2002). Violence against women is a well-recognized form of human women violation, and death is the most severe consequence of violence (Unol, et al, 2016). Characters of violence against women usually vary across countries and from one community to another. The data available about this phenomenon in Egypt are scarce. Great Cairo and Giza governorates are considered as a pool of Egyptian population from all other governorates in Egypt.
The aim of the present study is to assess the prevalence of violent women deaths in our community and throw light on the underlying factors that contribute to violent women deaths.
2. Subjects And Methods
A sample of adult women corpses, who died in suspicious circumstances, and autopsied in Zeinhommaurtory, Ministry of Justice by Forensic Medicine Authorities during 2011 and 2012 were chosen for the study Data were collected retrospectively from their medicolegal archives from the 1stof January 2011 to 31st of December 2012.
The data were statistically analyzed, in terms of socio-demographic characteristics, crime/death scene, time of death (month – wise, day/night time), causes and manners of death, the suspected perpetrators in homicidal cases and associated intoxications.
3. Results
Out of 3824 autopsied corpses of both sexes during 2011-2012, 317 (8.3%) adult women (>20 years old) were selected for the study.
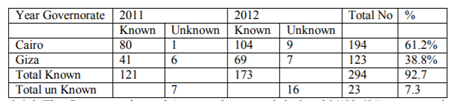
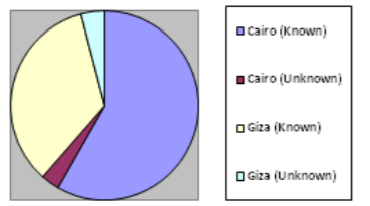
3.1.1. Identification of the Autopsied Women
All of them were Egyptians except two foreigners from Germany and Indonesia. The personal identity was known at time of autopsy for most of them (92.7%), and the unknown corpses were more from Giza than from Cairo. (Table -1) & (Figure. 1).
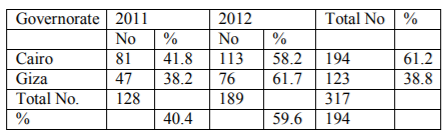
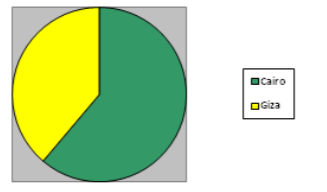
3.1.2. The Geographic Distribution of Autopsied Women
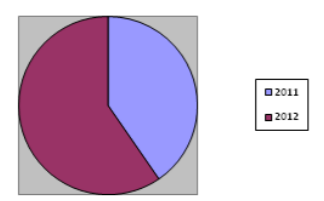
Cases drained from Cairo (61.2%) were more than those from Giza (38.8%) and those autopsied during 2012 (59.6%) were more than those during 2011 (40.4%) (Table- 2), (Fig. 2) & (Fig. 3).
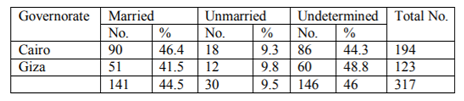
3.1.3. The Marital Status of Autopsied Women
It was known in (54%), out of them (44.5%) were married and (9.5%) were single, either divorced, widows or unmarried. The marital status could not be determined in (46%) of cases, as it was not mentioned in their archives (Table -3).
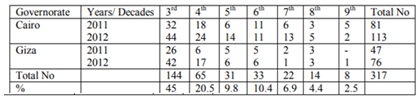
3.1.4. Age Distribution of Autopsied Women. (In Decades)
The majority of victims were at the 3rd decade (45%), followed by those at the 4th decade (20.5%). The number of cases decreased by increase of age, and a minority was found at the 9th decade (2.5%) (Table-4).
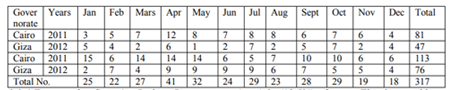
3.1.5. Date of Crime (Month/Wise) amongst the Autopsied Women
The number of autopsied women monthly ranged between 18-41 cases with a peak during April and May and smaller peaks during July, September and October, and a drop during November and December (Table -5).
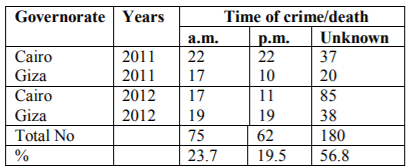
3.1.6. Time of Crime/ Body Discovery (Day/Night) among the Autopsied Women
Victimized women were discovered at day time (a.m.) in (23.7%) of cases and during night (p.m.) in (19.5%) of cases. The time could not be determined in most of cases (56.8%) as it was not mentioned in their archives (Table -6).
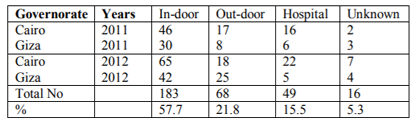
3.1.7. Scene of Crime/Death of the Autopsied Women
The corpses were found in-door in 183 cases (57.7%) and those found out-door were 68 cases (21.5%), Women who died in hospital during medical care were (15.5%) and the scene could not be determined in (5.3%) of cases (Table -7).
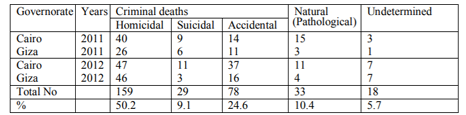
3.2.1. The Manner of Death in the Autopsied Women
About half of cases (50.2%) were homicidally killed (Femicide), and about quarter of them (24.6%) died accidentally, and suicidal deaths accounted to (9.1%) of them. Natural deaths due to pathological diseases contributed to (10.4%) of cases. The manner could not be determined in (5.7%) of cases either due to massive putrefaction or mutilation (Table -8).
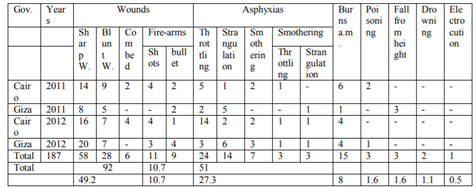
3.2.2. Causes of Death in Homicidal Cases (Femicides)
They accounted to (187) cases, about half of them were murdered by wounds (49.2%), mostly by sharp weapons. Violent asphyxias were diagnosed in more than quarter of them (27.3%), mostly by throttling, followed by strangulation and smothering alone or combined with either throttling or strangulation. Fire-arm injuries were encountered in (10.7%) of cases and ante- mortem burns in (8%). Few women were killed by either poisoning, fall from height, drowning or electrocution. Three victims of asphyxia showed signs of post-mortem burns and seven of them were thrown into water, 2 were thrown from height and 3 of them showed signs sexual assaults before death. Three cases proved by toxicological analysis to be intoxicated by CO gas alone or with alcohol, hashish or insecticide many cases showed multiple methods for homicides (Table -9).
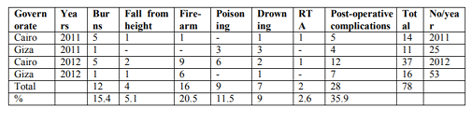
3.2.3. Causes of Death in Accidental Cases
Seventy-eight cases were found to die accidentally, by post- operative complications as hemorrhage or pulmonary embolism in (35.9%), Fire –arm injuries in (20.5%), flame burns in (15.4%), poisoning in (11%), drowning in(9%), fall from height in (5.1%) and road traffic accidents (RTA) in (2.6%) of them(Table -10).
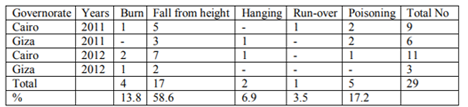
3.2.4. Causes of Death in Suicidal Cases
Cases from Cairo were (20) and from Giza were (9). Fall from height was found in more than half of the cases (58.6%), followed by poisoning in (17.2 %|) and flame burn in 13.8%. Two cases hanged them-selves, and one case was run – over by metro-train after being sexually abused (Table -11).
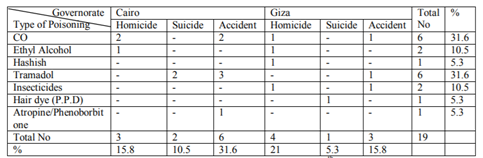
3.2.5. Types and Distribution of Poisoning in Autopsied Women
19 Cases out of 317 (6%) were found to be intoxicated. Poisonings by Co gas and tramadol were the commonest among them (31.6%) for each, followed by ethyl alcohol and insecticides
(10.5%) for each, then other poisons as hashish, hair dye (P.P.D), atropine, phenobarbitone (5.3%) for each of them. Homicidal poisoning was more from Giza, and accidental and suicidal poisoning were more from Cairo. Suicidal insecticide and hair dye poisoning were only from Giza. (Table-12).
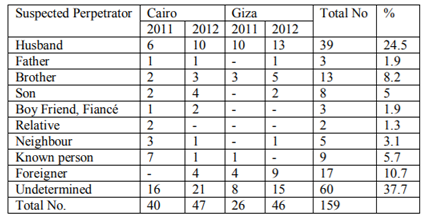
3.2.6. The Suspected Perpetrator in Femicide Deaths
The husband was the suspected perpetrator at time of autopsy in about quarter of homicidal cases (24.5%). Their number was more from Giza than from Cairo. In more than (1/3rd) of cases (37.7%) the suspected perpetrator was not determined. A foreigner was the assailant in more than 1/10th of them (10.7%) more from Giza than Cairo, to be followed by the brother (8.2%), a known person but not a relative, or a neighbor in (5.7%). The sons who killed their mothers constituted (5%) of cases. The father, boy-friend or fiancé or a relative represented the least proportion of suspected assailants (Table - 13).
4. Discussion
The autopsied women in the present study contributed to 8.3% of all the autopsied cases from both sexes during 2011 and 2012. This is considered a higher ratio if compared to the Istanbul study by, Unal, et al (2016) where they comprised only 2.6% of autopsied corpuses during 4 years period (2006-2010).
The socio demographic data showed that autopsied women from Cairo Governorate were more than those from Giza governorate (61.2 and 38.8% respectively), as the number of population in Cairo (24 districts) are more than those from Giza (11 districts). The incidence of violent women deaths was observed to be higher during 2012 than during 2011 in both studied governorates which may denote an increase of violence rate by time. This observation is in contradiction to the study in South Africa on autopsied women from 38 mortuaries that showed a decreased of incidence in 2009 below that reported 10 years before during 1999 (Abrahams, et al, 2013)
The majority of autopsied women in the present study were identified at time of autopsy (92.7%), and all of them were Egyptians except two foreigners from Germany and Indonesia. The identified corpses were more from Cairo than from Giza governorate as Cairo represents mostly an urban community, where identity cards are more regular than in the mostly rural communities as Giza.
The marital status of the autopsied women was determined only in (54.8%) of them due to deficient data in their archives. More than half of autopsied women were homicidally killed (Femicide). This finding may indicate that marriage does not protect from violent death. A higher prevalence was found in Portugal study by Periera, et al (2013), where intimate partner violence was the reason of homicide in 60.8% of all autopsied women.
As regards age distribution among the autopsied women (>20 years old), it was found that cases from the 3rd decade (20-30years) accounted to (45.4%) of autopsied women followed by those in the 4th decade (20.5%). The incidence decreased by the increase of age to a minimum at the 9th decade of life. Similar finding was reported by Nadia and El- barrany, (1994) by a similar study on smaller sample size (75 autopsied women). This finding indicates that violent death mostly occurs during the active stages of life (3rd-4th decades) rather than at later calm life. This result agrees with the study of Saeed, et al (2010), on suspected female homicide occurring between 2007-2009 in Faisalabad, as the majority of victims (75%) fall in the age range of 10-39 years (2nd, 3rd& 4th decades). This result also coincides with the study of Unal, et al (2016) in Turkey, where 49.7% of victimized women were between 21-40 years old.
Although the home is largely considered to be the safest place, the current study revealed that home (in – door) was the Commonest place of violence against women (57.5%), which was more than double the incidence of deaths out-door (21.5%). This result agreed with that of Unal, et al, (2016) who stated that the private residence was the commonest place of such violence (51.2%), while incidence in street-violence was only 14.5%. Similarly, the report from Costa Rica about femicide by Ana and Caba (2002) that stated that more than 70,000 women died in their own homes due to domestic violence.
The present study showed also that men (husband, father, brother, boy-friend or fiancé were the perpetrators in the majority of violent deaths in this series. Intimate partner violence (IPV) is a well-recognized phenomenon since many years, and men proved to be more likely to perpetrate nearly all types of violence, as masculinity is the root of violence (Fleming, et al, 2015). The study of Unal et al (2016), in Turkey, also proved that the husband was the perpetrator in 20% of autopsied women, and intimate partners comprised (52.3%) of perpetrators. In contrast to the present study, where no single female perpetrator was suspected, the study of Unal et al, showed that female perpetrators were involved in 4.4% of their demicide victims.
Month/wise distribution of autopsied women during the 2 years period of the study, showed that the peak incidence of deaths was during April and May. This result is consistent with that of Saeed, et al (2010) who found that the incidence of violent deaths was more in March, April and May during 2007, 2008 and 2009, which is the spring season in Punjab. However, the present study showed also, smaller peaks in July, September and October, which agree with the study of Andhra Pardaish, India by Mohanty, et al (2005) that showed a peak in winter. A previous study by Nadia and El-barrany (1994) showed a peak incidence at May, June, and July with a higher peak at December. It appears that there is no regular seasonal pattern for violence against women.
As regards the time of death (day/night) among the autopsied women, it was more during day/time (a.m.) (23.7%) than during night/time (p.m.) (19.5%). However, the real time of death could not be determined in more than half of the autopsied women (56.8%). These data were deficient in their archives. To the best of our knowledge, no reference mentioned information about time of violence against women. From the result of the current study, it may be concluded that violence during day activities is more than during night relaxation and sleep time.
The present work showed that about half of the autopsied women were murdered homicidally, followed by accidental then suicidal deaths. Similarly, in United States statistics of Department of Justice (2009) female homicides fell in (43%) between 1993 and 2007.
The same conclusion was reported by Nancy (2017), who found that homicide was the most common manner of death in autopsied women during 2014-2015 in the same mortuary (Zeinhom). The main cause of Femicide in the current study was wounds (49.2%) mostly by sharp weapons and to a lesser extent blunt weapons. This result is contrary to that of Nancy (2017) who found that homicide by blunt trauma was more than sharp weapon injuries. Violent asphyxia contributed to (27.3%) of femicides, while fire arm injuries comprised only (10.7%). The study of Mathew et al (2009) in South Africa showed that femicide by gun injuries were almost equal to femicide by blunt and sharp weapons, while the similar study in Srilanka by Colombo and Ragama, (2009) showed that fire-arm injuries mounted to 47% of extreme violence homicide. Also, the study of Unal, et al (2016), in Istanbul showed that fire-arm injuries contributed to (50.1%) of violent women deaths, while blunt trauma was (5%). The previous study done by the same author (Nadia and El- barrany, 1994) on a smaller sample (75 autopsied women), showed almost similar low incidence of fire-arm injuries (9.3%) as in the current study (10.7%).
In the present study, the accidental deaths were mostly due to post- operative complications, as hemorrhage or pulmonary embolism (35.9%), while accidental fire-arm injuries by uncontrolled shooting in celebrations, contributed to (20.5%) of accidental women deaths, which is rather higher than those of homicidal fire-arm deaths (10.7%. The commonest cause for suicidal women deaths in the present study was fall from height (85.6%), followed by poisoning (17.2%), then burns (13.8%). Similar results were reported by Nancy, (2017) in two years retrospective study (2014-2015) in the same Zeinhom morgue, Egypt. Cost Arica report (2002) stated that (58%) of women felt danger of dying in the hands of their aggressors and (47%) feel unsafe and considered suicide. Nevertheless, in the present study no homicide – suicide case was detected, in contrast to Istanbul study where seven out of 57 suicidal deaths committed suicide after homicide of their spouse.
Toxicological analysis of autopsied women in the current study proved that (19) cases out of (317) women were intoxicated by carbon monoxide (31.6%), and tramadol (opioid like) (31.6%) suicidally, accidentally or homicidally given.
Carbon monoxide was found to be the commonest poison by Nancy (2017), through a similar study. Ethyl Alcohol, tramadol and Hashish were detected in the studied autopsied women, which confirm the fact that the drugs of abuse are commonly associated with violence to overcome anxiety and/or depression of victims (Richardson &Fedr, 1996).
Insecticides and hair dye (Paraphenylene diamine) toxicity were detected only in autopsied women from Giza governorate where the rural agricultural products are available and easily accessible.
As regards the perpetrator in femicide cases, the present study showed that the husband was suspected in about quarter of them (24.5%), followed by persons of intimate relations as a brother, son, father, boy- friend or fiancé (17%) of cases. All the suspected perpetrators were men, mostly of intimate relations. Similar results were reported by other workers as (Nadia and El – barrany 1994),(Periera, et al 2013). (Nancy, 2017) and Also, reports from Australia, Canada, Mexico, Portugal, South Africa and U.S.A, stated that 40-70% of female murder victims were Killed by their intimate partner (U.N.D. (2008) (U.S. Depart (2009) and 3/2rds of victims of intimate partner or family related homicides were women (W.W. Violence against women (2015). However, the Istanbul study by Unal, et al, 2016), showed that (52.3%) of femicides were killed by victim’s spouses, but in (4.4%) the perpetrators were females. Men are more likely to be violent, as muscularity is mostly the root if violence, especially if they have lower income and education or abuse substances. (WHO, London, school (2010), (Fleming, et al, 2015).
5. Conclusion
• Violence against women is prevalent and is increasing in our community mostly against women whose age is in the 3rd decade of life.
• Femicide comprised about half the suspected women deaths during 2011-2012.
• Males only were the suspected perpetrators in the current study and no single female perpetrator was suspected.
• At home deaths by an intimate partner were more common and marriage did not protect from violent death.
• Wounds by sharp or blunt weapons were the commonest cause of death followed by violent asphyxias
• Fire-arm injuries were the cause of accidental rather than homicidal or suicidal women deaths, and their incidence is lower than other countries, perhaps because of the restrictions of gun- ownership by law.
• Fall from height was the commonest cause of suicidal deaths, followed by poisoning and burns
• Carbon monoxide gas and tramadol were the commonest poisons detected by toxicological analysis of autopsied women.
Recommendations
• Similar studies on larger sample are needed across other provinces to verify the nature, prevalence and risk factors of violence and put a suitable strategy to combat this tragic phenomenon.
• Computerization of victims achieves, including data on circumstances of death (ie. Time and place of death) to facilitate data recalling for legal and research purposes.
• Social awareness on gender- based and interpersonal violence consequences and draw-backs on individual and community safety and well – being is needed.
References
- Abraham, N., Mathews, S., Martin. L.J., Lombard, C., and Jewkes, R. (2009): Intimate partner femicide in South Africa in 1999 and 2009. Plos Medicine /www. Plosmedicine. Org., \April 2013/ Vol. 10/Issue 4/e1001412
- Ana, M. and Cabanas, C. (2002): FemicidioenCosta Rica: balance mortal https: //www research gate.net/ publication /2535 10913
- Colombo and Ragama- a study of Srilanka (2009): Extreme violence- homicide, an analysis of 265 cases from the office of JMO., Leg. Med. (Tokyo), 1: 363-365.
- European Union Agency for Fundamental Rights (2014): Fast- Facts, Statistics on violence against women and girls, virtual knowledge center to end violence against women and girls, www.endvawnow. Org> aeticles, 299
- Fleming, P.J, Gruskin, S., Rojo, F. and Dworkin, S.L. (2015): Men's violence against womenandmenareinterrelated: Recommendations for simultaneous intervention, social Sc. And Medicine, 146, 249-256.
- Krug, E.G., Dahiberg, L.L., Mercy, J.A., Zwi, A.B, Lozane, R. (2002): World report on violence and Health, chapter1, Violence a global publish health problem, P.3, WHO. Geneva.
- Mohanty, M.K, Kumar TS, Mohanram, A., and Palimar, V. (2005): Victims of homicidal deaths, and analysis of variables, J. Clin. Forensic Med., 12: 302 -304.
- Naida, A.K, and El–barrany, O.M (1994): Female victims of violence in Great Cairo city during 1993, in Proceeding of the 2nd Egypt. Int. Cong. Of Legal Medicine, P.61-68
- Nancy, M., Z. (2017); A descriptive medico- legal study of female deaths in Cairo Governorate, Egypt, in the 2nd Annual Congress of the International Association of Law and Forensic Science (IALFS), Jan. 17-19, Cairo, Egypt, P.O.R-13.
- Periera, A.R., Vieira, DN. And Magalhāes T. (2013): Fatal intimate partner violence against women in Portugal: a forensic medical national study, J. Forensic Leg Med., Nov.20 (8): 1099-1107
- Richardson J., and Fder, G (1996): Domestic violence: a hidden problem for general practice, Br. J. Gen. Pract, 405 (46), 239-242.
- Saeed, A., Paraveen, H., and Zafar, T. (2010): Fatal Homicidal violence against women and girls in Faisalabad, A.P.M.C vol: 4 No.2, July-December P.150-154.
- The World's Women (2015); Violence against women, Chapter (6), The United Nations, http://un status. Un. Org/unsd /gender> download
- Unal, EO, Koc, S., Unal, V., Akcan, R. and Javan, G.T. (2016); Violence against women: A series of autopsy studies from Istanbul, Turkey, J. of Forensic and Leg. Med. (40), 42-46.
- United States Department of Justice Statistics (2009): Ten Facts on Female victims of violence, supplementary Homicide Reports (SHR), Bureau of Justice Statistics (OJP), https//www justice. gov/ archives/opa/blog/10-facts-female-victims-violence.
- World Health Organization, London school of Hygiene and Tropical Medicine (2010): Preventing intimate partner and sexual violence against women: taking action and generating evidence. Geneva: WHO. Available: http://www.who.int/violence-injury-prevention/publications/violence/97892415640 07-eng.pdf.