


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Idiopathic Cyst, a Unilocular Cyst with Unknown Cause- A Case Report and Review
Shreyas Sorake1, Dr. Vijayendranath Nayak S2*, Raghavendra Kini3, Prasanna Kumar Rao4, Roopashri Rajesh Kashyap5, Gowri Bhandarkar5, Karthik M6
2.Consultant in Oral Medicine and Radiology, Viveka Dental Clinic, Mangaluru, Karnataka, India.
3.Professor and Head, Department of Oral Medicine and Radiology, A.J Institute of Dental Sciences, Kuntikana, Mangaluru, Karnataka, India.
4.Professor Department of Oral Medicine and Radiology, A.J Institute of Dental Sciences, Kuntikana, Mangaluru, Karnataka, India.
5.Reader, Department of Oral Medicine and Radiology, A.J Institute of Dental Sciences, Kuntikana, Mangaluru, Karnataka, India.
6.Lecturer, Department of Public Health Dentistry, Manipal College of Dental Science, Manipal, Karnataka, India.
Copyright : © 2019 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Traumatic bone cyst or simple bone cyst of the jaw is a very rare entity. It is usually seen during the routine radiographic examination. Etiopathogenesis of this cyst is still controversial. Usually traumatic bone cyst is devoid of epithelial lining. Here in we report a case of traumatic bone cyst in a 26 year old female.
Keywords: Traumatic bone cyst, Simple bone cyst, CBCT imaging.
1. Introduction
The term traumatic bone cyst was first used by Lucas in 1929 [1]. Traumatic bone cysts have been reported in the literature under a variety of names: Solitary bone cyst, hemorrhagic bone cyst, extravasation cyst, progressive bone cavity, simple bone cyst and unicameral bone cyst [2]. They are commonly found in the metaphysis of long bones, but are rare in the jaws [3]. Because of a lack of unique clinical and radiographic features, it is important to establish the differential diagnosis between traumatic bone cysts and other bone lesions of the jaws especially translucent lesions [4].
2. Case Report
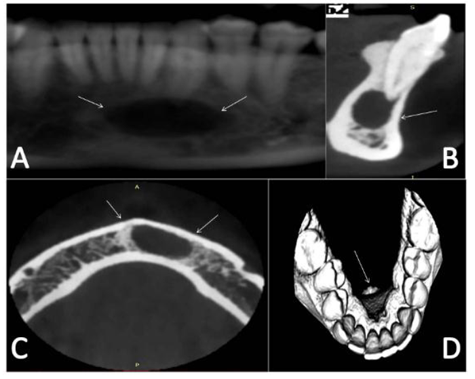
A 26 year old female patient was referred to the department of oral medicine and radiology for a Cone Beam Computed Tomography (CBCT) imaging as a pre operative requirement before undergoing a cosmetic surgery for the jaw. Past medical history and dental history of the patient was non contributory. CBCT of the jaws was performed which revealed unilocular osteolytic area on the parasymphysis region of the mandible, Involving the roots of the left mandibular canine (Figure.1A and 1B). Extension of the lesion was right mandibular incisors to the left mandibular canine (Figure1A). Axial section confirmed the extension of the lesion and revealed intact buccal and lingual cortical plates (Figure 1C). 3D image revealed prominent genial tubercles. A radiographic provisional diagnosis of Traumatic bone cyst was given (Figure 1 D). Vitality test was performed and confirmed that left mandibular canal was vital. Curettage of bony walls was performed. Specimen obtained from the curettage was sent for histopathological examination which revealed thin inflamed connective tissue lining the cavity composed of connective tissue and fibroblasts, osteocytes were evident in the lacunae and the final diagnois of traumatic bone cyst was given. Correlating the radiographic and histopathological findings a final diagnosis of traumatic bone cyst was given.
3. Discussion
Traumatic bone cyst is a rare bony lesion, non neoplastic, and asymptomatic innature. Traumatic bone cysts are considered almost exclusively lesions of the mandible, with a preference for the posterior areas (body and ramus) – although the symphysis may also be a site, like our reported case [5, 6]. They are classified by the World Health Organizationas part of a group of bone lesions that include the ossifying fibroma, fibrous dysplasia of bone, central giant cell lesions, aneurismatic bone cysts, and cherubism [7].
Many theories have been linked to the formation traumatic bone cyst which includes medullary bone haemorrhage secondary to trauma, cystic degeneration of fibro-osseous lesions, intraosseous vascular anomalies, alteration in metabolism of the bone and low grade infection [8]. It was suggested that trauma initiated a subperiostal hematoma that caused a compromised blood supply to the area, leading to osteoclastic bone resorption [9].
Radiographic investigations that can be carried out are Orthopantamograph and 3D imaging modality like Cone beam computed tomography and computed tomography, because of easy and accurate appreciation of typical radiographic appearance [10]. Traumatic bone cyst doesn’t cause resorption of the teeth roots. The cortical layer of bone or lamina dura may or may not be preserved. There is no loss of vitality of the tooth or at least there is no evidence that the tooth is non vital as a result of cyst growth [11].
Traumatic bone cysts generally show up as unilocular radiolucent areas in the posterior portion of the mandible; its margins are scalloped among dental roots. This radiographic pattern, however, may vary - the cyst may be multilocular, associated with unerupted/impacted teeth, and several cysts may be present in the same patient [12] were as in our reported case the cystic lesion was appreciated in anterior region of the jaw and was an unilocular lesion.
The differential diagnosis of radiolucent lesions to be considered are aneurismatic bone cysts, focal osteoporotic bone marrow defect, intraosseous vascular malformations, kerato-cystic odontogenic tumors, ameloblastomas, odontogenic myxomas, and central giant cell lesions. Although we found no association with unerupted/ impacted teeth in our sample, the keratocystic odontogenic tumor and the ameloblastoma were the most frequently mentioned tumors in the initial diagnosis, especially when the radiographic image showed a multilocular cyst [4].
The histology of traumatic bone cysts reveals only a connective tissue membrane lining the pathologic cavity, characteristic of pseudocysts. Cholesterol crystals, hemorrhagic foci, and osteoclasts may be found [9]. A few authors have reported the occurrence of multiple traumatic bone cysts and their association with fibrous/bony lesions such as the florid cemento osseousdysplasia especially in older patients[13]. The treatment of choice for traumatic bone cysts is surgery for curettage of the bone walls, which generally results in short term healing Recurrences, are rare, and usually occur within three months of surgery [14].
4. Conclusion
Traumatic bone cyst being accidental finding, it can be visualized during the routine radiographic examination carried out foreither orthodontic or orthognathic procedure, as in our reported case. Vitality test needs to be done for the tooth involved and ideally pulp therapy is beneficial. Thorough dental history or trauma history is very important before arriving to conclusion. At times the cause for the formation of cyst is unkown as in our case, during which radiographic diagnosis plays a major role. Since the etiology of this cyst is very unclear, so the term idiopathic cyst could be considered. Identification of such types of cysts and providing necessary treatment should be the primary goal of an oral physician.
References
- Lucas C, Blum T: Do all cysts of the jaws originate from the dental system. J Am Dent Assoc 1929, 16:659-61.
- Xanthinaki AA1, Choupis KI, Tosios K, Pagkalos VA, PapanikolaouSI.Traumatic bone cyst of the mandible of possible iatrogenic origin: a case report and brief review of the literature.Head Face Med. 2006 Nov 12; 2:40.
- Saito Y, Hoshina Y, Nagamine T, Nakajima T, Suzuki M, Hayashi T. Simple bone cyst. A clinical and histopathologic study of fifteen cases. Oral Surg Oral Med Oral Pathol. 1992; 74(4):487-91.
- Martins-Filho PR1, Santos Tde S, Araújo VL, Santos JS, Andrade ES, Silva LC. Traumatic bone cyst of the mandible: a review of 26 cases.Braz J Otorhinolaryngol. 2012 ; 78(2):16-21.
- Sapp JP, Stark ML. Self-healing traumatic bone cysts. Oral Surg Oral Med Oral Pathol. 1990; 69(5):597-602.
- Tong AC, Ng IO, Yan BS. Variations in clinical presentations of the simple bone cyst: report of cases. J Oral Maxillofac Surg. 2003; 61(12): 1487-91.
- Barnes L, Eveson JW, Reichart P, Sidransky D. WHO classification of tumours: head and neck tumours. Lyon: IARC Press; 2005.
- Blum T: Additional report on traumatic bone cysts. Oral Surg Oral Med Oral Pathol 1955;8(9):917-39.
- Baqain ZH, Jayakrishnan A, Farthing PM, Hardee P. Recurrence of a solitary bone cyst of the mandible: case report. Br J Oral Maxillofac Surg 2005; 43:333-5.
- Shetty SR, Mascarenhas R, Rao S, Rai G, Jose M, Rao PK. Preorthodontic CYST-report of a traumatic bone cyst diagnosed prior to orthdontic treatment. RevistaLatinoamericana De Ortodoncia y Odontopediatria. 2010:1-6.
- SebastijanSandev, KlaraSokler, Jonko Grgurevie. Traumatic bone cysts. ActaStomat Croat, 2001; 35: 417-20.
- Tong AC, Ng IO, Yan BS. Variations in clinical presentations of the simple bone cyst: report of cases. J Oral Maxillofac Surg. 2003; 61(12): 1487-91.
- Kuhmichel A, Bouloux GF. Multifocal traumatic bone cysts: case report and current thoughts on etiology. J Oral Maxillofac Surg. 2010;68 (1):20812.
- Baqain ZH, Jayakrishnan A, Farthing PM, Hardee P. Recurrence of a solitary bone cyst of the mandible: case report. Br J Oral Maxillofac Surg. 2005;43 (4):3335.