


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Localization of Inferior Alveolar Canal Through Cone Beam Computed Tomography
Bashir Ahmad Wani1*, Altaf Hussain Chalkoo2, Shazia Maqboo3
2.Professor, Department of Oral Medicine and Radiology, Government Dental College Srinagar, India.
3.Postgraduate Student, Department of Oral Medicine and Radiology, Government Dental College Srinagar, India.
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
The cone beam computed tomography (CBCT) considered as one of the most valuable imaging modality that enables three-dimensional reconstruction of images that are extremely reliable, allowing accurate assessment of the mandibular canal and its relations with other anatomical structures of the mandible. The material comprised of 115 CBCT scans, selected from a CBCT centre. The age of the patients ranged from 30 to 55years. The CBCT scans were used to evaluate the location of the mandibular canal from mandibular foramen to mental foramen, and classify its height in relation to the roots of the 1st and 2nd molars. Of the total 115 CBCT scans evaluated, there were 49 patients with the mandibular canals classified as type-1, 34 patients with type-II canals, 24 patients with type- III canals and 08 patients with type-IV canals having variations of asymmetric canals. Knowledge of the anatomy and anatomical variations of the mandibular canal with the path of inferior alveolar nerve is utmost important especially to perform various procedures in the area in order to minimize injury to the neurovascular bundle.
Keywords: Anatomy, Cone Beam Computed tomography, Mandibular Canal.
1. Introduction
The mandibular canal located within the mandible, an important anatomical landmark through which inferior alveolar nerve, artery and vein runs. The course of the canal begins in the mandibular foramen and ends at the mental foramen [1]. With the advancement of implants, the mandible is being widely used for implant reception site, therefore, anatomical knowledge of this region is extremely important for the success of implant procedures [2]. Due to increased surgical procedures and implant surgeries near third molar area, there are increased chances of injury to the inferior alveolar nerve, thereby causing temporary or permanent sensorial, tactile or thermal change [3].
Mandibular implants have an important role in the field of prosthetics, surgical and orthodontic procedures with success or failures directly related to the anatomical knowledge of this region as well as proper evaluation of bone quality [4] Mandibular canal has been widely studied with respect to their location, its path and possible variations in normal anatomy (Neves et al., 2009) [5].
In comparison to computed tomography, CBCT offers accurate 3-dimensional scanning with radiation doses that are lower, thereby enables its use in a normal clinical dental set-up [6]. The cone beam computed tomography considered as one of the most valuable imaging modality that enables three-dimensional reconstruction of images that are extremely reliable, allowing accurate assessment of the mandibular canal and its relation with other anatomical structures of the mandible [7].
The purpose of this study was to evaluate and assessment of the mandibular canal from the mandibular foramen upto the opening of mental foramen with its relation to the apices of second molar or first molar, if the former is absent and also with the inferior cortical border of the mandible using cone beam computed tomography (CBCT).
2. Material and Method
The material comprised of 115 CBCT scans, with age of the patients ranged from 30 to 55years. The CBCT scans were used to evaluate the shape of the mandibular canal from mandibular foramen to mental foramen, and classify its height in relation to the roots of the 1st and 2nd molars. Inclusion criteria include cbct scans of patients having the presence of the second molars bilaterally or in their absence first molars. Exclusion criteria include patients with pathological lesions or severe resorption of the mandible. CBCT images were obtained using NewTom VGi scanner (QR srl; Verona, Italy ) in standard resolution mode [palatal plane parallel to the horizontal plane, allowing the axial cuts parallel to the palatal plane with voxel size of 0.3mm], exposure parameters include kVp=110, exposure time of 3.6 s and FOV 8X8cm, or 8X12cm. Axial, Coronal and Sagittal cross sections with 1mm thickness at an interval of 0.5mm were prepared and reconstructions of the mandible to identify mandibular canal with its relation to the apices of the first or second molar and with the inferior mandibular cortex. Under the direct super-vision of a radiologist, images were evaluated by a trained post graduate student.
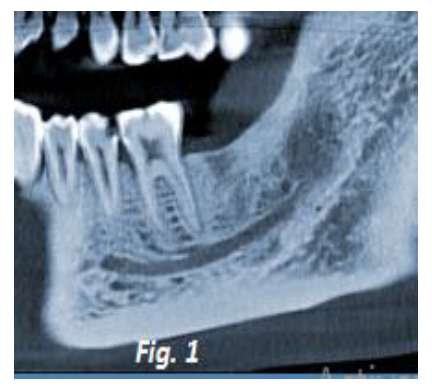
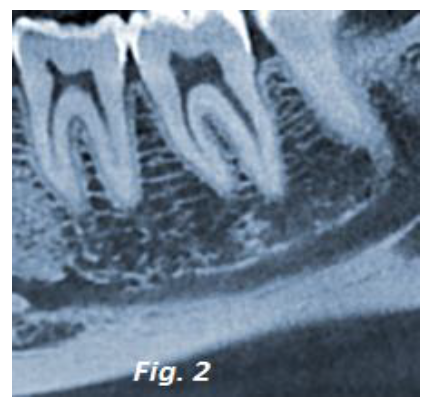
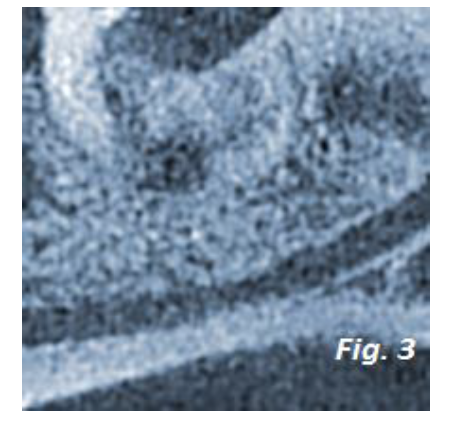
The measurements had been performed in the oblique sagittal plane. The parameters for classification of mandibular canal used was of Nortje et al. (1977): mandibular canals Type-I is a single, high, bilateral with a distance of up to 2 mm from the root apex of the mandibular second molar or the first molar (figure. 1), if the former is absent; Type-II is single, intermediate, bilateral with not fulfilling the criteria of type-1(figure. 2); Type-III is a single, low, bilateral, with a distance of up to 2 mm from the inferior cortical margin of the mandible (figure. 3), and Type- IV canals with variations including asymmetries, duplication or absence of mandibular canal.
3. Results
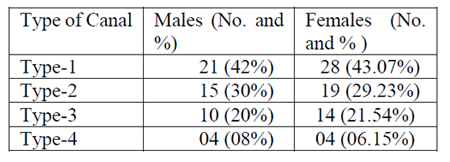
Of the total CBCT scans evaluated, there were 50 males (43.47%) and 65 females (56.52%) with the age range of 30 to 55 years. All the images evaluated presented with single, bilateral canals extending from the mandibular foramen to the mental foramen. There were 49 patients with the mandibular canals classified as type-1, 34 patients with type-II canals, 24 patients with type- III canals and 08 patients with type IV canals having variations of only asymmetric canals as shown in table-1.
4. Discussion
With the advances in technology, diagnostic techniques are allowing a thorough and accurate evaluation of body structures [8]. Among them, CBCT is an important tool for the accurate visualization of anatomic structures as well as pathologies in three dimensions with better resolution (Bueno et al., 2007) [9]. As there are advancement in implants with the mandible being widely used for implant reception site, anatomical knowledge of this region is extremely important for the success of implant procedures [2]. Due to increased surgical procedures and implant surgeries near third molar area, there are increased chances of injury to the inferior alveolar nerve, thereby causing temporary or permanent sensorial, tactile or thermal change [4].
Lindh, et al.(1995) had concluded that the tomographic examination surpasses the other radiographic assessment as it shows the mandibular canal with its relation to the cortical bone in a buccolingual direction [10]. Klinge, et al.[11] (1989) concluded that the most accurate location of the mandibular canal is provided by CT scan, as he measured the distance from the crest of the alveolar ridge to the mandibular canal roof in macroscopic sections and compared it with the distance obtained from various radiographs like periapical radiography, panoramic radiography, hypocycloidal tomography and CT images. One of the most common procedures in oral surgery is the extraction of third molars with many complications occuring if an adequate preoperative planning is not carried out [12]. CBCT images plays an important property of exactly determining the direction of the dislocation and extraction of molars, which cannot be done using only a panoramic radiograph [13].
In this study we evaluated the mandibular canal from the mandibular foramen upto the opening of mental foramen with its relation to the apices of second molar or first molar, if the former was absent and also with the inferior cortical border of the mandible using cone beam computed tomography (CBCT). We used the same parameters of panoramic radiographs (Nortjé et al.; Langlais et al., 1985; Devito & Tamburús, 2001) for the classification of mandibular canal [14]. We observed there was a higher prevalence of type I canals and the lowest was that of type IV canals, as was found by Nortje et al and Devito et al. Lins et al found similar results as observed in our study [15]. Sanchis et al. (2003)[16] and Rouas et al. (2007) [17] had found a double mandibular canal; Auluck & Pai (2005)[18] had reported a case of unilateral mandibular trifid canal, and Clays & Wackens (2005)[19] described a case of two mandibular canals, unilateral on right side, starting from the distinct mandibular foramina and ending in separate foramina.
Recent studies suggest that CBCT is the most reliable and accurate imaging modality for planning procedures in the area of the mandibular canal, in three dimensions with its relationship to the surrounding anatomical structures. With this, it is worth noting that the knowledge of the anatomy of mandibular canal with the path of inferior alveolar nerve is ut-most important especially to perform various procedures in the area in order to minimize injury to the neurovascular bundle.
5. Conclusion
Knowledge of the anatomy and anatomical variations of the mandibular canal with the path of inferior alveolar nerve is utmost important especially to perform various procedures in the area in order to minimize injury to the neurovascular bundle. CBCT is an important tool for the accurate visualization of anatomic structures as well as pathologies in three dimensions with better resolution.
6. References
- Butterfield KJ, Dagenais M, Clokie C. Linear tomography’s clinical accuracy and validity for presurgical dental implant analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84(2):203-9.
- McCollough CH, Zink FE. Performance evaluation of a multislice CT system. Med Phys. 1999;26(11): 2223-30.
- Adriana da Silva et al: COMPARATIVE STUDY OF SINGLE AND MULTISLICE COMPUTED TOMOGRAPHY FOR ASSESSMENT OF THE MANDIBULAR CANAL; J Appl Oral Sci. 2007; 15(3): 220-4.
- Hwang K, Lee WJ, Song YB and Chung IH. Vulnerability of the inferior alveolar nerve and mental nerve during genioplasty: An anatomic study. J Craniofac Surg 16: 10- 14, 2005.
- Neves, F. S.; Souza, T. C.; de-Azevedo-Vaz, S. L.; Campos, P. S. F. & Bóscolo, F. N. Influence of cone-beam computed tomography milliamperage settings on image quality of the mandibular third molar region. Oral Radiol., 30(1):27-31,2014.
- Bashir A, Altaf H.Chalkoo, Rizwan H. morphometric analysis of nasopalatine canal using cone beam computed tomography: PARIPEX - INDIAN JOURNAL OF RESEARCH, 2250-1991-2018
- Arellano, J. C. V. Computed tomography in the diagnosis and control of the TMJ malfunction treatment. J. Bras. ATM Oclusão Dor Orofac., 1(4):315-23, 2001.
- DelBalso AM, Greiner FG, Licata M. Role of diagnostic imaging in evaluation of the dental implant patient. Radiographics. 1994;14(4):699-719.
- Bueno, M. R.; Estrela, C.; Azevedo, B. C.; Brugnera Júnior, A. & Azevedo, J. R. Tomografia computadorizada cone beam: revolução na odontologia. Rev. Assoc. Paul. Cir. Dent., 61(5):354-63, 2007.
- Lindh C, Petersson A, Klinge B. Measurements of distances related to the mandibular canal in radiographs. Clin Oral Implants Res. 1995;6(2):96-103.
- Klinge B, Petersson A, MALY P. Location of the mandibular canal: comparison of macroscopic findings, conventional radiography, and computed tomography. Int J Oral Maxillofac Implants. 1989;4(4):327-32.
- Ohman, A.; Kivijärvi, K.; Blomback, U. & Flygare, L. Pre-operative radiographic evaluation of lower third molars with computed tomography. Dentomaxillofac. Radiol., 35(1): 30-5, 2006.
- Rood, J. P. Permanent damage to inferior alveolar and lingual nerves during the removal of impacted mandibular third molars. Comparison of two methods of bone removal. Br. Dent. J., 172(3):108-10, 1992.
- Nortjé, C. J.; Farman, A. G. & Grotepass, F. W. Variations in the normal anatomy of the inferior dental (mandibular) canal: a retrospective study of panoramic radiographs from 3612 routine dental patients. Br. J. Oral Surg., 15(1):55-63, 1977.
- LINS, C. C. S. A.; BELTRÃO, R. L. A.; GOMES, W. F. L. & RIBEIRO, M. M. Study of morphology of mandibular canal through computed tomography. Int. J. Morphol., 33(2): 553-557, 2015.
- Sanchis, J. M.; Peñarrocha, M. & Soler, F. Bifid mandibular canal. J. Oral Maxillofac. Surg., 61(4):422-4, 2003.
- Rouas, P.; Nancy, J. & Bar, D. Identification of double mandibular canals: literature review and three case reports with CT scans and cone beam CT. Dentomaxillofac. Radiol., 36(1):34-8, 2007.
- Auluck, A. & Pai, K. M. Trifid mandibular nerve canal. Dentomaxillofac. Radiol., 34(4):259, 2005.
- Claeys, V. & Wackens, G. Bifid mandibular canal: literature review and case report. Dentomaxillofac. Radiol., 34(1):55-8, 2005.