


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Myofascial Pain Dysfunction Syndrome: A Review
Nirupama. S1, Nishmitha J Suvarna1, Rashmi P V1, Preethi Poonja2*, Gowri P Bhandarkar3, Roopashri R Kashyap3, Prasanna Kumar Rao4,Raghavendra Kini5
2.Assistant Professor, Department of Oral Medicine and Radiology, A.J Institute of Dental Sciences, Mangalore, Karnataka, India.
3.Reader, Department of Oral Medicine and Radiology, A.J Institute of Dental Sciences, Mangalore, Karnataka, India.
4.Professor, Department of Oral Medicine and Radiology, A.J Institute of Dental Sciences, Mangalore, Karnataka, India.
5.Professor and Head, Department of Oral Medicine and Radiology, A.J Institute of Dental Sciences, Mangalore, Karnataka, India.
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
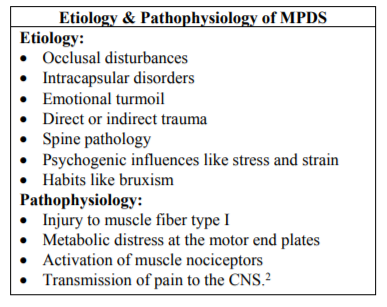
Myofascial pain dysfunction syndrome is one of the most common causes of chronic musculoskeletal pain. It is more common among young unmarried females. Various etiological factors include occlusal disturbances,intra-capsular disorders, emotional turmoil, direct or indirect trauma,spine pathology, psychogenic influences like stress and bruxism.The development of trigger point is considered to be one of the most important characteristic feature of MPDS. Clinical features include TMJ clicking sounds, impaired mandibular movement, trismus, preauricular pain, facial pain and jaw tenderness on function.Currently treating the underlying etiology is the most widely accepted treatment strategy which includes non-surgical and surgical management.
Keywords: Myofascial pain dysfunction syndrome, Preauricular pain, musculoskeletal pain, clicking sounds,Dental Science
1. Introduction
Myofascial pain dysfunction syndrome (MPDS) has always been an enigma, a big question mark. Some have even questioned the mere existence of MPDS; one might question if there is actually such a thing or it is just a myth created by the specialists [1]. It is more common among young unmarried females (married to unmarried ratio 1:2), withfemale to male ratio being 3:1. It occurs commonly between 15-35 years of age[3]. In the earlier centuries MPDS was attributed to the inflammation of fibrous tissues around the ligaments, tendons, muscles and periosteum of the stomatognathic system. But, now this syndrome has been defined as “dysfunction of the masticatory and associated muscles characterized by local pain and muscle stiffness”[1]. MPDS is one of the most common causes of chronic musculoskeletal pain. It does not cause any destructive changes in the temporomandibular joint. In fact, it is a psychological disorder which involves the masticatory muscles and results in pain, limitation in jaw movement, clicking sounds, jaw deviation and sensitivity in touching one or more masticatory muscles or their tendons.[2] However, various aspects of itsphysio-pathology, clinical manifestations and treatment remains unclear[3]. Treating the underlying etiology is currently the most widely accepted treatment strategy.
2. Etiology
There are multiple etiological factors for MPDS [Table1]. According to the psychophysiological theory, muscle spasm is a factor for myofascial pain dysfunction syndrome. Emotional factors are the primary etiological factors in stimulating chronic oral habits that produce muscle fatigue. Some complain of the pain immediately following a long dental appointment or the extraction of mandibular third molars. The presynaptic, synaptic and postsynaptic mechanisms of abnormal depolarization (i.e. excessive release of acetylcholine (Ach), defects of acetylcholinesterase and upregulation of nicotine Ach-receptor activity, respectively) have been proposed to be the possible etiological mechanisms[1].
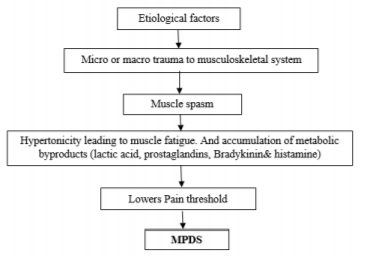
The unifying concept proposed by Lermank - holds that MPDS results from the interplay of an unbroken chain of etiological factors. The psychologic factors leads to an overall increase in masticatory muscle activity, while other factors such as occlusal and anatomic lead to selective increase in muscle activity (Flow chart 1)[2].
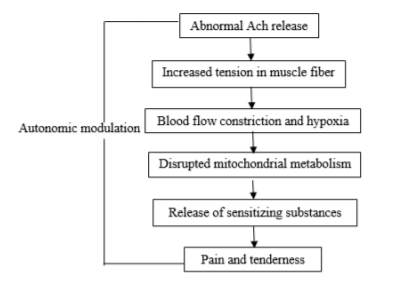
Myofascial trigger points requires a self-sustaining positive feed-forward process. Simons presented the integrated hypothesis for myofascial trigger points to offer an explanation for the same. It is a six- link chain starting with the abnormal release of acetylcholine which causes increased muscle fiber tension, seen as the taut band found in a myofascial trigger point. This taut band constricts the blood flow that leads to local hypoxia. The reduced oxygen disrupts mitochondrial energy metabolism thereby reducing ATP and leading to tissue distress, release of sensitizing substances. The activation of nociceptors (pain receptors) causes pain and also lead to autonomic modulation which potentiates the abnormal acetylcholine release (Flow chart 2)[2].
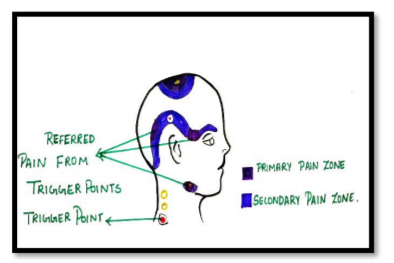
The development of trigger point is considered to be one of the most important characteristic feature of MPDS.Trigger points are small exquisitely tender areas, which causes pain to the distant region, called the Referred Pain Zone. They are activated by pressure, movement, change of barometric pressure and tension (physical or emotional). Trigger points differ from “Tender spots” (TS’s) in the sense that the pain of TS’s are localized in the vicinity of the spot while trigger point pain refers to a distant area. However, the treatment of trigger points and TS’s are exactly the same.
3. Taut Band
It is the group of tense muscle fibres extending from a trigger point to the muscle attachments, the tension being caused by contraction knots that are located in trigger point region[1].
Clinically MPDS is usually associated with unilateralpain [Table 2]. In some cases, pain can be bilateral but it need not be symmetrical. The quality or character of the pain reported by the patient most often will fall into three gross categories:
• Category I: A dull-aching pain,
• Category II: A sharp-shooting pain (burning), and
• Category III: A tight-drawing sensation[1].
4. Laskin’s Diagnostic Criteria
Laskin has proposed 4 cardinal signs and negative characteristics for MPDS.
1) Four cardinal signs
• Unilateral pain
• Muscle tenderness
• Clicking or propping noise in the TMJ
• Limitation of jaw movement
2) Negative characteristics
• No radiographic evidence
• No tenderness in TMJ area on palpation via the external auditory meatus
5. Differential Diagnosis
• Cluster headache: Cluster headaches are a series of relatively short but extremely painful headacheevery day for weeks or months at a time.
• Migraine headache: Migraine headache is a result of specific changes within the brain. It causes severe head pain that is often accompanied by sensitivity to light, sound, or smells.
Post herpetic neuralgia: Postherpetic neuralgia (PHN) is nerve pain which occurs due to damage to a peripheral nerve caused by the reactivation of the varicella zoster virus (herpes zoster, also known as shingles).
• Temporal cell arteritis: Giant-cell arteritis (GCA), also called temporal arteritis, is an inflammatory disease of blood vessels.
• Trigeminal neuralgia: Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, which carries sensation from your face to your brain.
• Middle ear infection: An ear infection (acute otitis media) is most often a bacterial or viral infection that affects the middle ear, the air-filled space behind the eardrum that contains the tiny vibrating bones of the ear[5].
6. Management
MPDS is managed by non- surgical and surgical methods.
a) Diet: Elimination of hard and chewy food helps to reduce loading forces on the joints and to rest hypertonic jaw muscles.
b) Rest: Each patient should be made aware of the relationship between stress and muscle tension. Resting the jaw is possible by making the patient aware of their unconscious postural, swallowing, clenching or grinding habits.
c) Pharmacological therapy includes,
• Analgesic drugs: Opioid analgesics depresses CNS, just relieve pain. Whereas, non-opioid analgesic relief pain without depressing CNS. Examples- morphine, pethidine, codeine, salicylates and paracetamol.
• Anti-inflammatory agents: Commonly used are salicylates (aspirin), propionic acid (ibuprofen), acetic acid (indomethacin), fenamic acid, oxicam, aryl-acetic acid derivatives (diclofenac sodium).
• Anxiolytics agents: Benzodiazepines such as alprazolam, diazepam, lorazepam and oxazepam are commonly used to alter the patient’s perception of reaction to the supportive therapy.
• Muscle relaxants: Commonly used are carisoprodol, chlorzoxazone, meprobamate, methocarbamol and cyclobenzaprine.
• Herbal medicines: Lavender, lemon balm, rosemary, kava kava, skullcap are some of the recommended medicines[1]
• Anticonvulsants: Gabapentin, Pregabalin
• Antidepressants: Tricyclic antidepressants, Sumatriptan, Duloxetine4
d) Other Methods
• Transcutaneous Electric Nerve Stimulation (TENS)
• Electrical Twitch Obtaining Intramuscular Stimulation (ETOIMS)
• Magnetic Stimulation (MS)
• Laser Therapy[4]
e) Non Pharmacological
• Dry needling: Dry needling is a treatment that involves a very thin needle being pushed through the skin to stimulate a trigger point.
• Manual therapy: Manual therapy is a commonly used treatment for MPS as it has been considered as one of the most effective techniques for the inactivation of MTrPs. It includes deep-pressure massage, stretch therapy with spray (where a taut band is stretched immediately after cold spray), superficial heat and myofascial release[4].
Condylotomy: Condylotomy is an osteotomy (a controlled fracture) performed through the condylar neck/vertical mandibular ramus.
• High Condylectomy
• Menisectomy: Menisectomy is the surgical removal of all or part of a torn meniscus
• Myotomy: Myotomy describes a surgical procedure in which muscle is cut.
• Arthroscopy: Arthroscopy is a surgical procedure orthopaedic surgeons use to visualize, diagnose, and treat problems inside a joint.
• Botulinum toxin A (BtA) injection[2]
7. Conclusion
Myofascial pain syndrome is a type of muscle pain syndrome associated to trigger points. It has a defined pathophysiology that leads to the development of characteristic taut or hard band in muscle that is tender which refers pain to distant sites. It is generalized once it is chronic. But Myofascial pain syndrome can resolve with ideal treatment regimens. However, many patients with myofascial pain syndrome have symptoms for years. Outcomes are best when a multifaceted treatment approach is done.
References
- Arora, Pooja, Goswami, Roma, Raman, Shrimant, Jain, Pulkit. The Enigma of Myofascial Pain Dysfunction Syndrome. International Journal of Advances in Scientific Research 2015; 1(01): 01-04
- Reji R, Krishnamurthy V, and Garud M. “Myofascial Pain Dysfunction Syndrome: A Revisit.” Journal of Dental and Medical Sciences 2017;16(1):13-21
- Garg, et al. : Myofascial Pain Dysfunction Syndrome : An Overview-Heal talk, July- August 2013; Volume 05 Issue 06: Page 12-14
- Desai MJ, Saini V, Saini S. Myofascial Pain Syndrome: A Treatment Review. Pain and Therapy. 2013; 2(1):21-36.doi:10.1007/s40122-013-0006-y.
- Anitha A, Babu N. A, Sankari S. L, Malathi L. Myofacial Pain Dysfunction Syndrome - A Review. Biomed Pharmacol J 2016;9(2).827-828