


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
The Reconstruction of the Mandibular Continuity Defect by Nonvascularized Rib Graft : About two Cases
Ouattara B1,Koffi KM2,Harding MB3,Bissa HC4,Kone R5,Garba I6,Bouletreau P7
2 Department of radiology, CHU Yopougon (RCI).
3.Department of stomatology, maxillo-facial, plastic and the face surgery CHU-Lyon Sud (France).
Copyright : © 2017 Miguel C L. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
We often come across mandibular continuity defect in corrent practice. They are the result of traumatical, infectious, tumoral and abnormalcy pathologies. The treatment of such a case is nowadays well codified requiring bony drafts, endoprothesis and osteogeonic distraction.
We describe our experience of two clinic cases of continuity defect of mandibular reconstruction by nonvascularized ribgraft. In the two cases withsome respectives retreat of twelve and twenty-three months, the results were satisfactory by taking into account the functional and esthetical aspect
Keywords: Reconstruction – mandibular – traumatism – tumor – graft,Dental Science,Dental
1. Introduction
The anatomical reconstruction of mandibular continuity defectis not an easy task for the surgeon to cope with because of the complexity in the working of the mandibular and the specificity related to the treatment of lesions which affect the neck and face segment [1, 2]. These defects bring about some aesthetical, functional (chewing, swallowing, speech, phonation, respiratory) and so social consequences.
In developed countries with the advent of microanatomosistissular transfert technics (or free laps) in the neck and face area started in 1970s. The management of these defects is well structured [1 - 4]. That is not the case in our medically underserved countries where those mandibular continuity defects represent serious problems of reconstruction affecting considerably sick men socio professional reinsertion.
We report our experience on two cases of mandibular continuity defect reconstruction by non-vascularized ribgraft.
2. Our Observations
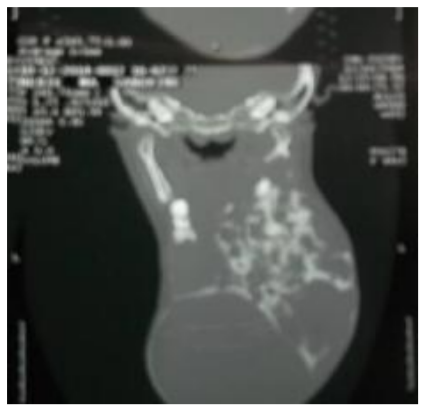
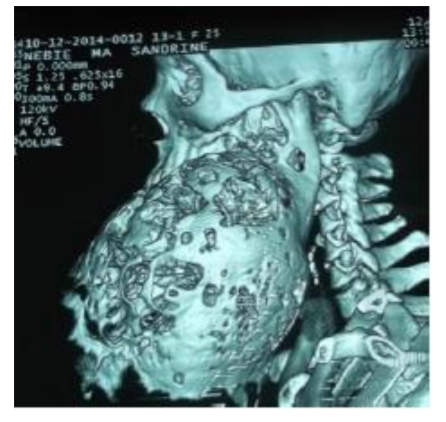
A 30years patient (woman) who has been consulted suffering from avoluminous mandibular tumor which has started developing since ten years. The sympathology would have been started by a left angulomandibular oncosis which increased gradually. Everything combined in a painless context with mobilities, migration and spontaneousloss of teeth. The patient had previously started using a traditional medication based on plant decoction application and sudstance meant to be inhaled on vapour and over and steel didn’t recover from her pain. The clinical analysis of the inside omouth revealsa volumous left mandibular tume faction exceeding the median line by giving "double head" aspect, covered by aglossy skin, painless of heterogenous consistency with an hypothesia in the area of ipsilateralmandibular nerve and a lack of neck and face adenopathy(figure 1& 2).


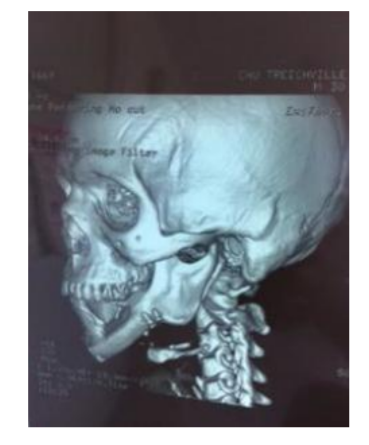
Inside the mouth analysis we noticed an open mouth by the tumor which was covered by an anetoderma made of nmerousvenous maze carryingantagonist teeth print. Dental check-up brought to light some migration and some dental mobilities from thirty-five to forty-six with lack of left inferior group of back teeth. In paraclinicsphere, the CT brought to light an osseous fenestrum of polygeodic images occupying all the left semi mandibular other passing the median line and extending till forty-six, and in 3D …reconstruction we noticed some images in "beenest" (figure 3& 4).
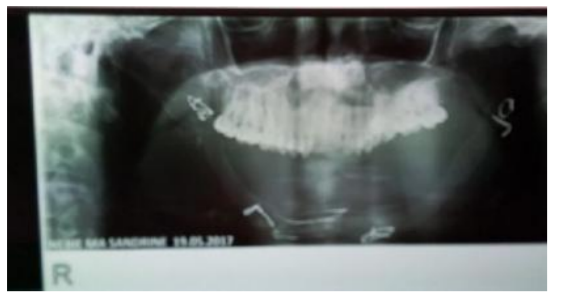
In doing so we suspected a benign tumor and a surgery instruction had been given. A continuity resection had been realized for this patient at the right angular level with dissarticulation at left, realizing a defect of "T" type followed by an immediate metalic endoprosthesis reconstruction (figure 5, 6 & 7).

After the surgery an ameloblastoma was found. Ten months later we have seenour patient for a metallic endoprosthesis and non-vascularized two free osseous ribgraft reconstruction taking at the fifth and sixth rib level and conform according to the form of defect to be reconstruct (figure 8).

The patient had been regularly treat, at eleven months we observed a good osseous graft and we proceeded to a prothetic rehabilitation by an amovible prothesis, allowing the restauration of the facial balance (figure 9,10,11).


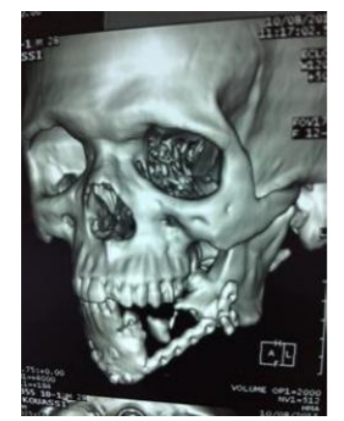
A 32 years patient (man), victim of ballistic traumatism which causes a mandibular continuity defect in a type of "La". He was taking into charge initially by ametallic endoprosthesis reconstruction with feeble parts repair. The patient consulted us for a bonegraft reconstruction. The outside mouth clinic analysis revealed a left lower cheek depression and a left lip and chin anaesthesia. Inside the mouth analysis we noticed a limitation of 30mm while opening the mouth and alack of tooth from 31 to 37. The CT realized showed a mandibular defect from the median line to the left preangular area, reconstructed by ametallic endoprosthesis (figure12).
For this patient we have made a reconstruction of mandibular by a ribosseous free graft with the fifth right rib. The evolution was satisfied with a retreat of twenty-three months(figure13&14).

3. Discussion
The aims of the construction are morphologic, also functional with the ability to open and close the mouth. The primary reconstruction is always desirable in order to obtain best results. It exists different procedures
It consistin replacing the mandibular defect by a bigblotch or splint in titanium or its alloys like temporary space or definitive.
It is based on the concept of bonee longation thanks to a distractor put inside the mouth. The progressive traction practising with in the osseous fragment send an osteogenous in the interfraction under the periosteum activity. The osteogenous distraction is able to treatat the same time the associate integument retraction that allows prothetic dental implant rehabilitation.
- The osseous auto grafts that can be either free nonvascularized or free vascularized [5- 7].
Cariou [8]distinguish five types of mandibular defect according to their past or lateral situation which determine the priority of osseous reconstruction.
- Type A with subdivision in :
- "Aa" Defect limited to the symphysis area.
- "Ab" Defect spread to the whole man dibulararch from angle to angle.
- Type L with subdivision in :
- "La" Defect limited to the horizontal branch.
- "Lb" Defect increase to a semi-mandibular with or without the mandibular condyle.
Mandibular continuity defect beyond a semi-mandibular and causing bone length problem to bring.
In the two cases showed we noticed a defect of type T and another of type "La". The continuity defect of mandibular care is well codified in developed countries call on micro anastomosislap. At ours because of the lack of ressources we are always obliged to use nonvascularized graft. Before doing this reconstruction we must do a deep pre surgery check-up which is composed of :
* Bones which permit to determine exactly the volume and the morphology of the defect to be reconstructed.
* local factors around bones are covering tissue which will help to isolate the reconstruction of septic place inside the mouth and of the dental ouside place.
* an accurate dental check-up shall be done.
* Intercurrent factors : They modify the local conditions of the recontruction (X-ray therapy, dental local infectious focus, active or quiescents osseous or growing site activity and the pediatric periosteum must be respected).
* General factors( age, sex, mental condition and cooperation that we should expect from the patient, nutritional condition, metabolic condition, cardio respiratory condition, lifestyle and exeresis adjuvant treatment.
* Aetiology factors (benign or malign tumoral pathology, traumatic pathology, osteoradionecrosis and osteitic pathology). According to literature all continuity defect superior to 8 cm need a reconstruction by microanastomosis lap for both patients. The continuity defect extended beyond 8 cm and the recontruction had been done by non-vascularized ribgraft. After the different surgeries the results have been satisfied with good grafts on respectives retreat of 13 and 23 months. For the partisan of such grafts, the interestis in its test facility and its weak morbidity [9,10].
4. Conclusion
Continuity defect of mandibular represents a complex decisonal process for the surgical team. It always deals with particular case to which we must take into account the interest of the patient. We must continually take into consideration the satisfaction of the surgeon when he reconstructs mandibular and the happiness of the patient.
If in medically served countries the reconstruct-ion through micro anastomosis graftis well appropriate, the use of nonvascularized free grafts always constitute a credible alternative in our skies.
References
- Braga-Silva J, Jarger MRO, Favalli PPS. Reconstruction mandibulaire : les lambeaux micro-chirurgicaux de crete iliaque et péroné. Annales de chirurgie plastique esthétique 50 (2005) 49-55.
- CordeiroPalgo GA. Conceptual considérations in mandibular reconstruction. Clin Plast Surg 1995; 22(1) :61-9.
- Albert S, Guedon C. Chirurgie reconstructrice par lambeaux micro-anastomés en cancer ologiecervico-faciale. La lettre du cancerologue vol XX n 2, Fevrier 2011 : 116
- Kim JW, Hwang JH, Ahn KM. Fibularflap for mandible reconstruction in osteora dionecrosis of the jaw : selection criteria of fibulaflap. Maxillo facial Plastic and reconstructive Surgery (2016) 38-46.
- Benhalima H, Kamal D, Boulaich M, Kzadry M. reconstruction des pertes de substances interruptrices de la mandibule chez l’enfant. Annales Odonto-Stomatologiques n 251, septembre 2010 : 271-76.
- Peri G, Blanc J-L, Mondie J-M, Cheynet F, Lepoutre F. La reconstruction des pertes de substances interruptrices de la mandibule. XXXIe congrès de stomatologie et de chirurgie maxillo-faciale. Marseille du 19 au 22 septembre 1989. Masson éditeur, Paris.
- Urken ML (1991). Composite free flap in oromandibular reconstruction. Review of the literature. ArchOtolaryngol Head Neck Surg 117 : 24-32.
- Cariou JL, Payement G, Rochebiliere A, Bellavoir A. Le choix du transplant libre compose avec os dans la reconstruction des pertes de substances interruptrices de la mandibule. A propos de 28 cas. Ann Chir Plast Esthet 1994 ;39 : 449-460.
- James DR, Irvine GH. Autogenous ribgrafts in maxillo-facial surgery. J.Maxillofac. Surg. 1983,11 :201-203.
- Laurie SWS, Kaban LB, Mulliken JB, Murray JE. Donor-site morbidity after harvesting rib and iliacbone. Plast. Reconstr. Surg. 1984,73 : 933-938.