


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Considerations Regarding Preparation for Porcelain-fused-to-metal Crowns
Claudia Florina Andreescu1, Andreea Mariana Banateanu2, Diana Eugenia Radulescu3
Copyright : © 2017 Miguel C L. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Full-coverage crowns are most frequently recommended prosthetic restorations in many clinical situations. Conventional porcelain-fused-to-metal crowns are most ordered full-coverage crowns to private dental laboratories. The aim of this study is to assess the quality of dental preparations for porcelain-fused-to-metal crowns made by dentists in private practice. The following aspects are considered: total occlusal convergence angle, incisal or occlusal reduction, axial reduction, presence of undercuts, aspect of cervical line, existence of sharp lines or angles and presence of supplementary retention. A detailed look at all aspects regarding tooth preparation can help to improve clinical results in everyday practice.
Keywords: porcelain-fused-to-metal crown, abutment preparation, working cast, error, Dental Science, Dental
1. Introduction
Full-coverage crowns are most frequently recommended prosthetic restorations in case of extensive coronary destruction, trauma, and treatment of partial edentulous span [1].
In order to achieve long-term success of prosthetic restorations is essential adequate preparation of supporting teeth. Goodacre et al [2] suggest respecting following principles in tooth preparation for coverage crown: 10-20 degree of total occlusal convergence (TOC) and 0.5-1 mm of axial reduction for metallic crowns and 1-2 mm of axial reduction for porcelain-fused-to-metal (PFM) and all-ceramic crowns.
Quality of tooth preparation is influenced by occlusal reduction, axial reduction, occlusal convergence, aspect of cervical preparation and axial walls. There are many studies that analyse the quality of tooth preparation for coverage crowns done by students [[3]-[5]], dentists [6], residents [5] or specialists [7]. Majority of these evaluates TOC, neglecting other aspects of preparation, which are most commonly errors denounced by dental laboratories [8].
Conventional PFM crowns are used form more than 30 years due to their advantages: strengths and aesthetics and are most ordered full-coverage crowns to private dental laboratories [9].
The aim of this study is to assess the quality of dental preparations for PFM crowns made by dentists in private practice. The following aspects are considered: TOC angle, incisal or occlusal reduction, axial reduction, presence of undercuts, aspect of cervical line, existence of sharp lines or angles and presence of supplementary retention.
2. Materials And Methods
Assessment of tooth preparation can be done intraorally or by viewing the impression before sending to the laboratory or checking the stone or scanned model. The most accurate method is assessment of model because allow evaluation from all angles by direct visual inspection[10].
There were examined 120 working models and 201 preparations from three different dental clinics after cementation of crowns or bridges. 94 models with 137 preparations for PFM crowns were selected.
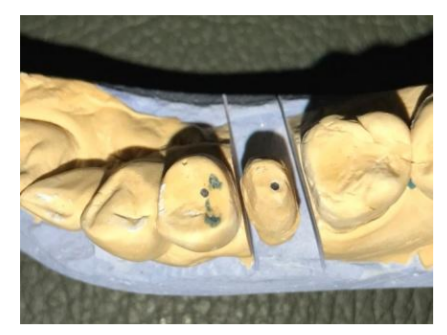
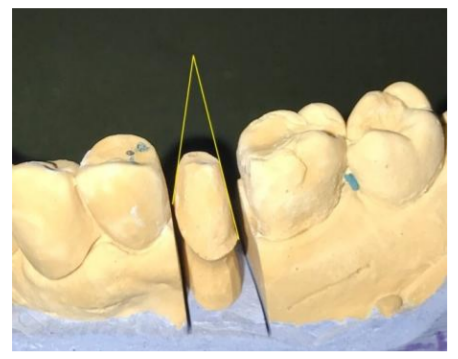
All models were examined with 2.5 magnification from occlusal (with and without antagonists), buccal and oral aspect (Figure 1-2) and photographed. Two lines (mesial and distal) were drawn from cervical margin parallel with prepared surface on each photographed preparation with the purpose to measure mesio-distal TOC angle (Figure 3).
• mesio-distal TOC angle,
• incisal or occlusal reduction was appreciate as adequate (A) when respected tooth morphology and there was no marking signs from laboratory or inadequate (I),
• axial reduction was appreciate as adequate (A) when respected tooth morphology and there was no marking signs from laboratory or inadequate (I),
• aspect of cervical line was appreciate as adequate (A) when was smooth and clearly or inadequate (I),
• presence (classified as inadequate I) or absence (classified as adequate A) of undercuts,
• presence (classified as inadequate I) or absence (classified as adequate A) of sharp lines and/or angles.
• presence (P) or absence (A) of supplementary retention.

3. Results And Discussion
There were evaluated 137 preparations for PFM crowns made for incisors 56 (40.87%), canines 14 (10.22%), premolars 28 (20.44%) and molars 39 (28.47%).
Mean value of mesio-distalTOC is 26.54° (Table1). Incisal or occlusal reduction is adequate in 62.77% cases, axial reduction in 54.01%, undercuts are present in 12.41% preparations examined, cervical finish line is inadequate in 37.96% and sharp lines and/or angles are found for 21.17% preparations (Table 2). Supplementary retention is present just in one preparation (0.73%).
A good preparation is essential for a well-adapted crown. One causes of crown failure is lack of retention and primary retention of crown is dependent of tooth height and occlusal convergence. The TOC value is more than the value recommended by prosthetic books, but similar findings were reported by different studies [7, 11,12]. However, there is no statistically significant difference of retention between 12° TOC and 20° TOC for a full coverage crown preparation on premolar [13].
An adequate incisal/occlusal reduction is important for crown and tooth resistance, this reduction should be enough for crown fabrication, but respecting tooth morphology and consequently tooth longevity. It was frequently present absence of functional cusp bevelling, which could lead to thin crown or deficient occlusal contacts [14]. Axial reduction is often inadequate on lingual surface of incisors, where is not respected preparation in two different plans. Similar fact is reported also for all-ceramic crowns [[8],[15].
Presence of undercuts impedes insertion of the crown and requires adaptation. Incomplete or uneven finish line determines deficiencies in marginal adaptation that may lead to ceramic fracture.
Supplementary retention is indicated for short teeth to improve retention and TOC should be less than 20° [16].
Errors in tooth preparation could appear due to: lack of experience, poor access, visual errors and anatomical variations.
4. Conclusions
This study reveals errors in tooth preparation for PFM crown like: inadequate incisal or occlusal reduction, inadequate axial reduction, presence of undercuts, deficient finish line, and existence of sharp lines and/or angles.
A detailed look at all aspects regarding tooth preparation can help to improve clinical results in everyday practice.
References
- Steele JG., Wassell RW, Walls AWG.Changing patterns and the need for quality.British Dental Journal 2002; 192: 144–148.
- Goodacre CJ, Campagni WV,Aquilino SA. Tooth preparations for complete crowns: an art form based on scientific principles. J Prosthet Dent.2001; 85(4): 363-76.
- Okuyama Y, Kasahara S, Kimura K. Quantitative evaluation of axial wall taper in prepared artificial teeth. Journal of Oral Science 2005; 47(3):129-33.
- Rafeek RN, Marchan SM, Seymour KG, Zou LF, Samarawickrama DY. Abutment taper of full cast crown preparations by dental students in the UWI School of Dentistry. Eur J ProsthodontRestor Dent. 2006 Jun; 14(2):63-6.
- Dorriz H, Nokar S, BaghaiNaini R, Madadi A. The Convergence Angle of Full-coverage Crown Preparations Made by Dental Students. Journal of Dentistry. 2008 5(1): 37-41.
- Patel PB, Wildgoose DG, Winstanley RB. Comparison of convergence angles achieved in posterior teeth prepared for full veneer crowns. The European Journal of Prosthodontics and Restorative Dentistry. 2005; 13(3):100-4.
- Khalil Al Ali, Khalid A. Al Wazzan, Mohammad D. Al Amri, Abdul-Majeed Al-Shahrani, Mohammed Al-Shahrani, Al-Qahtani H. Assessment of convergence angle of full veneer preparations carried out by practitioners with different levels of experience. The Saudi Dental Journal. 2009; 21(1): 37-44.
- Adams D. The ten most common all-ceramic preparation errors: a doctor/technician liaison's perspective. Dentistry Today 2004; 23(10): 94-99.
- Andreescu CF. Assessment of Impression Techniques for Crowns and Bridges. Annals of Prosthodontics and Restorative Dentistry 2015; 1(1):5-8.
- DiTolla M. Common preparation mistakes that cost you money. Dental Economics 15 May 2015; 105(5).
- Madani A, Ghahramanloo A, Shokati M. Assessment of convargece angles of tooth preparation for porcelain fused to metal restorations by general dentists. JBUMS.2001; 13:51-56.
- Al-Moaleem MM, Al Hashim NS, Asiri KA, Al Makhloti EA, Al Ahmari NM, Tikare S. Assessment of Porcelain Fused to Metal Crown Preparations by General Practitioners in Saudi Arabia. British Journal of Medicine and Medical Research.2015;7(2), 116-23.
- Vinnakota DN. Effect of preparation convergence on retention of multiple unit restorations-An in vitro study. Contemporary Clinical Dentistry. 2015, 6(3): 409-13.
- Syed S, Al-Moaleem MM, Shariff M. The quality assessment of teeth prepared by fresh graduates for ceramo-metal full coverage crowns. The Saudi Journal for Dental Research. 2016; 7(1), 24-28.
- Al-Dwairi ZN, Al-Hiyasat AS, Aboud H. Standards of teeth preparations for anterior resin bonded all-ceramic crowns in private dental practice in Jordan. Journal of Applied Oral Science.2011, 19(4), 370-7.
- Jayna M, Jayna A, Yadav B, Dabas N. Clinical insight into tooth preparation: An update. Saint Int Dent J 2015; 1: 2-7.