


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Paper or Plastic? A Foreign Body Ingestion Leading to Small Bowel Obstruction. A Case Report
Thomas Kerestes MD1*, D. James Smith MD1
Copyright : © 2019 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: The ingestion of a foreign body is a common event. It most often occurs in young children. When ingestion occurs in adults, it is usually incidental. Individuals with psychiatric disorders, patients with dentures, and those with alcohol dependencies are more likely to ingest a foreign body accidentally. Other adults are known to ingest fish or chicken bones accidentally. The majority of ingested foreign bodies pass through the gastrointestinal tract without any complications. The minority of ingested foreign bodies will require endoscopic intervention while only ~1% require surgical intervention.
Case Description: A 91-year-old female with late-stage dementia presented with abdominal pain and vomiting of 1-day duration. Computed tomography obtained in the emergency room was suggestive of partial small bowel obstruction vs. ileus. She was treated conservatively with bowel rest. After 48 hours of failed medical management, she was taken to surgery. Exploratory laparotomy identified a firm, mobile mass in mid jejunum. Surgeons performed a small bowel resection. The specimen when opened revealed a tightly compacted sheet of plastic. Postoperative the patient did well and recovered without any complications.
Conclusion: This incident is the first report of a mechanical small bowel obstruction caused by ingestion of a plastic bag. Our report highlights the practice of using multiple window-computed tomography views when evaluating a patient with intestinal obstruction.
Paper or Plastic, Foreign Body, Ingestion Leading,Small Bowel Obstruction, Clinical Case Reports.
1. Introduction
The ingestion of a foreign body is a common event. It most often occurs in young children. When a foreign body is ingested by an adult, it is often incidentally ingested while concurrently eating food. However, it has also been shown to be more common with individuals who have psychiatric disorders, are alcoholics, and patients who wear dentures [1-4]. In children, the most commonly ingested items include objects commonly found on the ground such as coins or batteries. In adults, the most commonly ingested foreign bodies include fish or chicken bones as well as toothpicks. Most ingested foreign bodies, up to 80% reported, successfully pass through the gastrointestinal tract without complications. Approximately 20% of reported incidents required endoscopic intervention while 1% required surgery. [5-14] Often, the patient is unaware of the actual ingestion. In our case our patient was an elderly female with late-stage dementia whom unknowingly swallowed a portion of a plastic bag which subsequently lead to a small bowel obstruction. To our knowledge, there has not been a reported case with a similar outcome.
2. Case Description/Summary
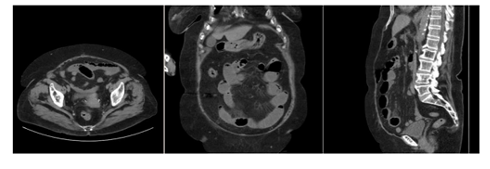
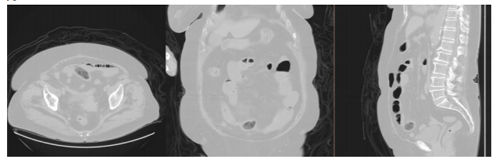
A 91 year old female with late stage dementia presented to the emergency department with acute onset of abdominal pain and vomiting. Her son, with whom she lives, provided most of the medical history. She had one episode of vomiting the prior to arrival. Her vomitus was brown in color and provided no relief of her pain. She had a normal bowel movement later in the day but continued to have pain. She was able to tolerate a small breakfast the morning of presentation without any issues. She stated that she has been passing some flatus. Her past medical history is significant for multiple abdominal procedures in the past, including a procedure secondary to a previous small bowel obstruction ten years ago, the extent of the procedure was unknown by the patient. On physical exam, her abdomen was soft, mildly distended, tender to palpation across the lower abdomen, and without peritoneal signs. A CT of the abdomen/pelvis was obtained which was suggestive of obstruction. No mass was mentioned or identified at this time. The decision was made to conservatively treat her for partial small bowel obstruction vs. ileus. She was placed in observation, IV fluid hydration, NPO. At this time, she was not complaining of nausea and the use of nasogastric tube was deferred. She was given dulcolax suppository and continued with conservative management for the next 48 hours with serial abdominal exams. Her symptoms remained unchanged as she continued to have abdominal distension and tenderness. A small bowel follow-through was obtained which showed an obstruction with no filling of the colon. At this time a decision was made to proceed to the operating room. A midline exploratory laparotomy was performed. Upon entry to the abdomen a small number of adhesions to the omentum and small bowl were noted. The small bowel was dilated, but otherwise appeared grossly normal. Proceeded to inspect the small bowel from ileocecal valve to ligament of treitz. A large firm mass was identified in the mid jejunum with decompressed loops of bowel distally. The distal loops of bowel were tethered to one another with loose adhesions. Attempts were made to milk the mass proximally and distally which proved purposeless. The decision was made to resect that portion of bowel and perform side to side anastomosis. The specimen was opened on the back table and the foreign body appeared to be a tightly compacted large sheet of plastic. This was sent to pathology which later would confirm that it was part of a plastic shopping bag. Now knowing that there was a foreign body causing obstruction the imaging was again reviewed. The foreign body is not perceptible using the standard abdominal view (Figure 1). By switching the view to a lung window, the foreign body became distinctive (Figure 2). The foreign body which can be seen on the CT using the lung window view coincides with the approximate location which it was uncovered intra-operatively. Postoperatively she did well and was discharged home without any complications.
3. Discussion
Our patient presented with a working diagnosis of adynamic ileus vs. partial small bowel obstruction. Due to her baseline cognitive status, there was a delay in the diagnosis of foreign body ingestion due to the fact that she did not recall the episode. One study reported a foreign body was identified within two to six days[1,4]. We were unable to verify a timeline of ingestion. Conservative management was initiated on admission. Subsequently a small bowel follow-through was obtained which revealed a small bowel obstruction, no barium was present in the large bowel. At this time decision was made to proceed to surgery. Obtain operative exploration the obstructing mass was located in the small bowel. Upon resection of the affected portion of the bowel, a mass was found to be a large sheet of plastic. There did not appear to be any evidence of perforation prior to surgery. However, the small bowel is the more common site in the gastrointestinal tract for perforations to occur. These perforations are usually caused by long, elongated, or sharp objects[15,16]. Although intestinal perforation can also be caused due to impaction which subsequently leads to bowel ischemia. This type of perforation is often subclinical and not detected on routine imaging[15,17]. Postoperatively, our patient had appropriate return of bowel function. She was unaware of how the sheet of plastic was ingested.
4. Conclusion
This is the first report of a mechanical small bowel obstruction caused by ingestion of a plastic bag. Treatment began with conservative management as the mechanical obstruction was not identified at initial onset. Once the patient failed conservative management the situation became surgical. An exploratory laparotomy with small bowel resection was performed. Ultimately, the patient recovered without any adverse sequela. This case demonstrates how multiple window views on computed tomography can display different entities and assist in the diagnosis of intraluminal foreign bodies and intestinal obstruction.
References
- Komninos and Tsiligianni Journal of Medical Case Reports 2010, 4:244 http://www. Jmedical case reports .com/content/4/1/244
- Cheng W, Tam PK: Foreign-body ingestion in children: experience with 1,265 cases. J Pediatr Surg 1999, 34(10):1472-1476.
- Velitchkov NG, Grigorov GI, Losanoff JE, Kjossev KT: Ingested foreign bodies of the gastrointestinal tract: retrospective analysis of 542 cases. World J Surg 1996, 20(8):1001-1005.
- Selivanov V, Sheldon GF, Cello JP, Crass RA: Management of foreign body ingestion. Ann Surg 1984, 199(2):187-191.
- Ambe P, Weber SA, Schauer M, Knoefel WT: Swallowed foreign bodies in adults. Dtsch Arztebl Int 2012; 109(50): 869−75. DOI:10.3238/arztebl.2012.0869
- Webb WA: Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc 1995; 41: 39–51.
- Cheng W, Tam PK: Foreign-body ingestion in children: experience with 1,265 cases. J Pediatr Surg 1999; 34: 1472–6.
- Ginsberg GG: Management of ingested foreign objects and food bolus impactions. Gastrointest Endosc 1995; 41: 33–8.
- Ikenberry SO, Jue TL, Anderson MA, et al.: Management of ingested foreign bodies and food impactions. Gastrointest Endosc 2011; 73: 1085–91.
- Smith MT, Wong RK: Foreign bodies. Gastrointest Endosc Clin N Am 2007; 17: 361– 82.
- Eisen GM, Baron TH, Dominitz JA, et al.: Guideline for the management of ingested foreign bodies. Gastrointest Endosc 2002; 55: 802–6.
- Mosca S, Manes G, Martino R, et al.: Endoscopic management of foreign bodies in the upper gastrointestinal tract: report on a series of 414 adult patients. Endoscopy 2001; 33: 692–6.
- Ngan JH, Fok PJ, Lai EC, et al.: A prospective study on fish bone ingestion. Experience of 358 patients. Ann Surg 1990; 211: 459–62.
- Zhang S, Cui Y, Gong X, et al.: Endoscopic management of foreign bodies in the upper gastrointestinal tract in South China: a retrospective study of 561 cases. Dig Dis Sci 2010; 55: 1305–12
- Nicolodi GC, Trippia CR, Caboclo MFFS, Castro FG, Miller WP, Lima RR, Tazima L, Geraldo J. Intestinal perforation by an ingested foreign body. Radiol Bras. 2016 Set/Out; 49(5):295–299.
- Ziter FM Jr. Intestinal perforation in adults due to ingested opaque foreign bodies. Am J Gastroenterol. 1976;66:382–5.
- Pinero Madrona A, Fernández Hernández JA, Carrasco Prats M, et al. Intestinal perforation by foreign bodies. Eur J Surg. 2000;166: 307–9.