


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Pseudallescheria Boydii Keratitis
(Scedosporium Apiospermum)
Raj Yashwanth1*, Anuja1, Suneetha2, Manoharbabu1
2.Department of microbiology, Aravind eye hospital, salem, Tamilnadu,India.
Copyright : © 2019 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
We describe a patient with Pseudallescheria boydii keratitis. The treatment of mycotic keratitis remains difficult This case demonstrates that identification and susceptibility testing should be rapidly performed. In cases of indolent keratitis, the possibility of fungal infection should be kept in mind.
Fungal Keratitis, Pseudallescheria Boydii, scedosporium apiospermum
1. Introduction
Fungal keratitis is most common among ag-ricultural workers in rural tropical areas [1]. Pseud-allescheria boydii is a widespread fungus known to cause opportunistic human infection, usually associated with trauma [2]. Fungal keratitis generally occurs in patients with diabetes who have metabolic acidosis, but it can also occur in patients who are immunocompromised due to treatment with steroids, lymphoma, renal failure, or chemotherapy.
We describe a patient with P boydii keratitis who had no documented history of trauma or immunodeficiency Unidentified minor trauma could have been the cause of this case. We also review the clinical spectrum of P. boydii in noncompromised patients and discuss the treatment modalities in this particular case.
2. Case Report
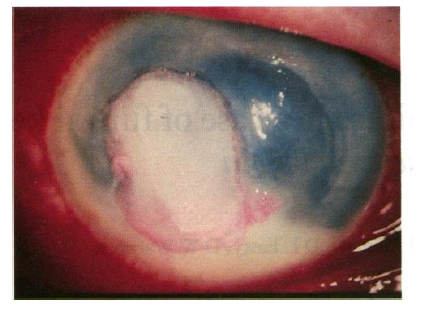
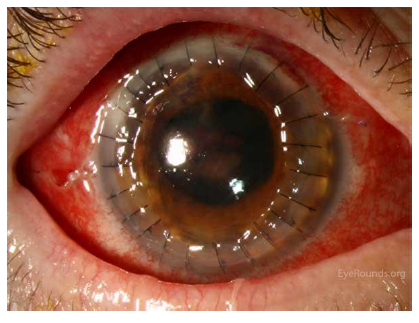
A 40 year old female presented with a keratitis in the right eye. Three days earlier, an unwashed glass-particle had hit her right eye in a glass recycling factory. Initially it caused only minor discomfort, but the situation deteriorated over a three day period and a painful red eye with poor vision developed. Visual acuity was reduced to 6/60. Slitlamp examination showed a central corneal ulcer with indistinct elevated margins and a surrounding ring- shaped stromal infiltrate. There was marked anterior chamber inflammation with 3mm hypopyon. We performed a first corneal scraping, which was negative for bacteria and fungi. Intensive treatment with topical Natamycin (5%), broad spectrum antibiotics and cycloplegics was started. A repeated scraping revealed a large amount of filamentous fungi on GIEMSA staining. Debridement of the necrotic corneal tissue was performed and treatment was modified to topical voriconozole (1%) hourly and oral Itraconazole 400 mg daily. Three weeks later, the causative fungus was identified as Pseudallescheria Boydii. We added topical Amphotericin B (0.15%) hourly. Despite the intensive and broadspectrum treatment, a progressively enlarging corneal infiltrate was noticed after an initial period of improvement. A penetrating keratoplasty was performed five weeks after the initial injury. Microscopic examination of the excised cornea showed infiltration by multiple septate filamentous fungi in the middle and deep stromal layers, with an overlying necrotic and acute non-granulomatous inflammatory infiltrate and an intact but folded Descemet’s membrane. Topical Natamycin 5% qds and topical steroids were continued for one month after surgery. The Itraconazole tablets were continued for two months on a tapering schedule. This treatment eradicated the fungal infection. One and a half year later on examination, visual acuity was 06/12 and showed a clear corneal graft, a quiet anterior chamber and some posterior capsular opacities.
3. Discussion
Pseudallescheria Boydii is found throughout the world in soil, decaying organic substances and water. It is a very rare cause of filamentous fun-gal keratitis. The first report of Pseudallescheria Boydii was made in 1955 and since then only fourteen cases have been described in world literature [1,3,4,5,7].

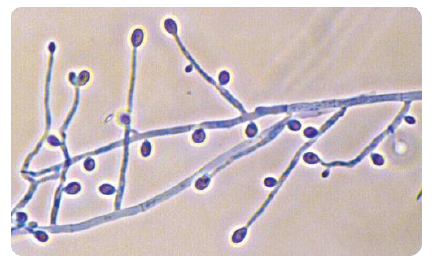
Scedosporium apiospermum Colonies are fast growing, greyish-white, suede-like to downy with a greyish-black reverse. Numerous single-celled, pale-brown, broadly clavate to ovoid conidia, 4-9 X 6- 10 um, rounded above with truncate bases are observed. Conidia are borne singly or in small groups on elongate, simple or branched conidiophores or laterally on hyphae. Conidial development can be described as annellidic, although the annellations (ring- like scars left at the apex of an annellide after conidial secession) are extremely difficult to see. Optimum temperature for growth is 30-37°C. RG-2 organism.
Ascocarp formation may be stimulated on cornmeal agar or other nutrient deficient media, however it should be noted that many isolates may fail to produce cleistothecia. Cleistothecia (non-ostiolate ascocarps) are yellow-brown to black, spherical, are most- ly submerged in the agar and are composed of irregularly interwoven brown hyphae. When crushed cleistothecia release numerous, faintly brown, ellipsoidal ascospores, 4-5 X 7- 9 µm in size. A Graphium synanamorph may also be present.
The teleomorph is currently referred to as Pseudallescheria boydii, however as all species of Pseudallescheria have Scedosporium anamorphs, it is presumptive to use the teleomorph name to describe this fungus without seeing cleistothecia (ascocarps). Until the taxonomy of Pseudallescheria is resolved, it is recommended that laboratories use the anamorphic name Scedosporium apiospermum when describing this fungus.
In 1979, the Food and Drug Administration approved the clinical use of broad spectrum anti- fungal agents like Natamycin and Miconazole. These drugs were used in the five most recent case reports of Pseudallescheria Boydii keratitis. In two of these five cases, still an enucleation was required [1,3]. This was most probably due to the intensive use of corticosteroids prior to the diagnosis of fungal involvement: diminished host resistance by steroids allows deep invasion of fungi. If a history of trauma by vegetable matter is present, fungal keratitis should always be considered and the use of corticosteroids avoided. The presence of filamentous fungi is easily missed because of the relative absence of fungi in the superficial stromal layers, and the difficulty of culturing them. Therefore repeated, vigorous corneal scraping and/or corneal biopsy is required to confirm a suspected fungal keratitis. The treatment of fun- gal keratitis remains a challenge for each ophthalmologist. At present Natamycin is the recommended first line drug [2]. In deeper fungal infections and those not responding to Natamycin, additional topical therapy, such as Miconazole and Amphotericin B, is required. Pseudallescheria Boydii, however, is often considered to be resistant to Amphotericin B, but the frequency with which this occurs is not well de-scribed [6]. Antifungals are hydrophobic and thus poor penetration of topical antifungals is the rule. Therefore the routine use of systemic antifungals, in particular Itraconazole and Fluconazole, is justified in severe or deep keratitis. Even with optimal medical therapy surgical intervention may be required to eradicate the infection: such measures may include debridement, keratectomy with conjunctival flap and penetrating keratoplasty [2].
References
- BLOOM P.A., LAIDLAW D.A.H., EASTY D.L., et al. − Treatment failure in a case of fungal kera- titis caused by Pseudallescheria Boydii. Br J Oph- thalmol 1992; 76: 367-368.
- KAUFMAN H.E., BARRON B.A., MC DONALD M.B. − The Cornea. 2nd ed. 1998. Newton: Liese- gang. Fungal keratitis: 231-241.
- MILLS R., GARRETT G. − Pseudallescheria Boy- dii keratitis. Australian and New Zealand J Oph- thalmol 1992; 2: 253-256.
- PAUTLER E., ROBERTS R.W., BEAMER P.R. − Mycotic infection of the eye. Monosporium Apios- permum associated with corneal ulcer. Arch Oph- thalmol 1955; 53: 385-389.
- RUBEN S. − Pseudallescheria Boydii keratitis. Acta Ophthalmol 1991; 69: 684-686.
- WALSH T.J., PETER J., MC COUGH D.A., et al. − Activities of Amphotericin B and antifungal Azoles alone and in combination against Pseu-dallescheria Boydii. Antimicrobial Agents and Chemotherapy 1995; 39: 1361-1364.
- ZAPATER R.C., ALBESI E.J. − Corneal Mono- sporiosis. A review and report of one case. Oph- thalmologica 1979; 178: 142-147.