


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Case Report of Osteopenia of Prematurity
Yara Salameh1, Rami George Maalouf1, Hani Waked1, Georges Nicolas1
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is a case report that discusses a very low birth weight premature infant, born at 29 weeks of gestation, presenting a severe and resistant hypocalcemia. She was diagnosed with rickets of prematurity, which is a rare and asymptomatic disease.
Case Report, Osteopenia, Prematurity,Clinical Case Reports1. Introduction
Nowadays, neonatologists are facing an important challenge: osteopenia or rickets of prematurity, and that’s because of the increased advances in intensive care and survival of preterm infants[1,2]. Osteopenia of prematurity appears at three to twelve weeks of age.
Although its exact incidence is difficult to quantify, it has been increasing; 20 to 30% and 50 to 60% in infants below 1500g and 1000g respectively (4). To prevent the osteopenia of prematurity, many risk factors have been detected: long-term diuretics or corticosteroids use, phenytoin, immobilization, deprivation of intrauterine minerals supply, prematurity (28 weeks of gestation), birth weight, insufficient intake of vitamin D and calcium in postnatal period, decrease in fetal movements, parenteral nutrition and neonatal pathologies such as sepsis and necrotizing enterocolitis[2].
In the beginning of the disease, the majority of the infants are asymptomatic. However, screening is primordial due to late-term complications; long bones and rib fractures. At four weeks of life, laboratory findings most commonly reveal features such as low serum Calcium, Phosphore < 1.8mmol/L, elevated ALP >500UI/L, tubular renal reabsorption of phosphate (TRP)> 95% showing also the sufficiency of P supplement elevated bone – specific ALP (B-ALP) at eight weeks of age [1,3,4]
In addition to this, a urinary Ca 1.2mmol/l and Ph 0.4mmol/l[1]. The radiological markers are not to be forgotten. Old fractures and cortical thinning, widening of the epiphyseal plate on a wrist radiograph later when BMC decreases to 20%-40% [2]. However, the use of Dexa scan and QUS are limited because of their limited availability and high cost.
Recent studies showed that rickets of prematurity is associated with a lower number of thymidine-adenine (TA) repeats polymorphism of the estrogen receptor gene.
Enteral P supplementation should be started with a dose of 75 to 140 mg/kg/day in addition to 150 to 220mg/kg/day of calcium. If it fails, ergocalciferol therapy should begin with a minimum dose of 200 to400IU daily depending on the weight of the infant. (1,4) Premature infants who do not tolerate human milk fortifiers should start with supplements of calcium and phosphorus.
2. Case Presentation
The patient reported is an infant, born by c-section delivery at 29 weeks of gestation due to the rupture of a meconial amniotic sac, presenting with severe and resistant hypocalcemia. The child had a weight of 1,22kg putting her in the category of very low birth weight (VLBW). Apgar score at delivery was 5 at 1 minute and 9 at 5 minutes. The newborn girl was diagnosed with hyaline membrane disease. She then developed respiratory depression, was intubated and admitted to the NICU. Chest X- ray showed diffuse infiltrates and antibiotic was started.
At 71 days of age, the patient developed a severe asymptomatic hypocalcemia. Upon further investigations, she had negative family history of hypocalcemia, deficiency in Vitamin D, rickets, osteogenesis imperfecta and other diseases that can cause hypocalcemia.
On physical exam, the patient did not develop any sign of hypocalcemia such as seizures, tetany, loss of muscular contractility, muscle cramps and spasms, facial twitching etc. Also, the patient did not present any signs and symptoms of pathological fractures.
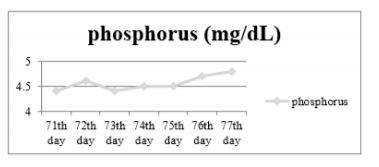
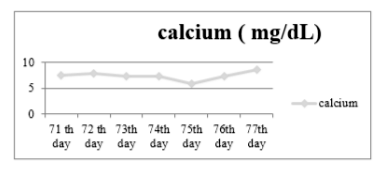
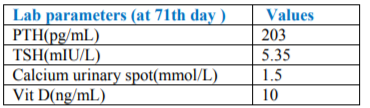
Calcium gluconate was started for three days with no improvement.The patient was seen, then, by an endocrinologist who suspected osteopenia of prematurity. Supplements of calcium and vitamin D were added to the treatment at the 75th day. Laboratory work up was done on the 71th day (Table 1). Calcium and phosphorus were assessed on a daily basis. The correction of the calcium (Graph 2) and phosphorus (Graph 1) level was achieved after the beginning of supplementation with vitamin D.
To conclude, this patient was diagnosed with osteopenia of prematurity which is a rare and asymptomatic disease with late-term complications. Thus, it is often undiagnosed in premature babies. However, the patient had multiple risk factors such as aspiration of meconium, hyaline membrane disease and prematurity putting her at risk of developing rickets of prematurity.
References
- Metabolic bone disease of prematurity Clin.Transl.Endocrinol.2014 Sep; 1(3): 85– 91doi: 10.1016/j.jcte.2014.06.004
- Moghis Ur Rehman and Hassib Narchi Metabolic bone disease in the preterm infant: Current state and future directions World J Methodol. 2015 Sep 26; 5(3): 115–121 doi: 10.5662
- Hitrova S, Slancheva B, Popivanova A, Vakrilova L, Pramatarova T, Emilova Z, Yarakova N.
- Osteopenia of prematurity--prophylaxis, diagnostics and treatment 2012; 51(7):24-30
- Duygu Besnili Acar, Sultan Kavuncuoğlu, Merih Çetinkaya, Ercüment Petmezci, Mesut Dursun, Orhan Korkmaz, Emel Kayrak Altuncu Assessment of the place of tubular reabsorption of phosphorus in the diagnosis of osteopenia of prematurity Turk Pediatri Ars. 2015 Mar; 50(1): 45–50. Published online 2015 Mar 1. doi: 10.51 52/tpa.2015.147