


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Pulmonary Artery Thrombus Presenting as Cyanotic Cardiac Defect in a Neonate
Dr Sumita A Jain, Dr Laxman Aggarwal, Dr Kaknale Harish Kumar, Dr Deshraj Chawla, Dr Mohit Badgurjar, Dr Rajeev, Dr Rajneesh, Dr Bharthi Mohan
Copyright : © 2016 Jain SA. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Sliding Inguinal hernia with ovary as its content is very rare in elderly female. Here we present a case 70 year old female who presented with swelling in the both groin associated with dragging pain in the left iliac fossa. She was investigated and diagnosed clinically as bilateral indirect inguinal hernia. Bilateral Hernioplasty was planned. On left side it was sliding inguinal hernia with ovary as its content.
Keywords: Indirect Inguinal Hernia, Ovary
1.Introduction
Inguinal hernia is uncommon in females compared to males. Incidence rate being 1.9% the ratio of boys to girls is 6:1.The site of presentation being 68% in right side, 23.4% on left, and 8.5% BLATERAL. The reported incidence of its occurrence is 71% in children under 5 years and 30% in adolescents or women in reproductive age group and 2.9% exclusively in elderly. In elderly women, indirect hernias are more common than direct hernias and typically occur during age 40–60. Most of these hernias contain intestinal contents and rarely viscera such as female adnexa (ovaries or fallopian tubes) in 3% of hernia cases.
2.Case Report
A 70 year old female presented with bilateral groin swelling, right side groin swelling since 5 years and left side since 1 and half years with dull aching pain in both groin since 1 year. Past medical history was insignificant. Obstetric history included eight vaginal deliveries (P8L7A0D1); tubal ligation was done 28 years back, attained menopause 25 years back. Local examination revealed a reducible swelling in her both inguinal region with positive cough impulse and deep ring occlusion test suggesting the indirect inguinal hernia.
Except routine test, no other tests were done.
Patient was operated first for right side as she didn‟t give consent for bilateral mesh hernioplasty. Open Lichtenstein's hernia repair was done after ligating & excising the sac .Patient was on follow up and admitted again for left inguinal hernia repair after 3 months. She was taken for Lichtenstein repair. On operation it was found to be sliding inguinal hernia with ovary as it content. As ovary was viable it was reduced and Lichtenstein"s repair done after excising the redundant sac. Post op period was uneventful and pt. discharged on post op day 4.
Figure1 .Pre Op – Bilateral Inguinal Hernia

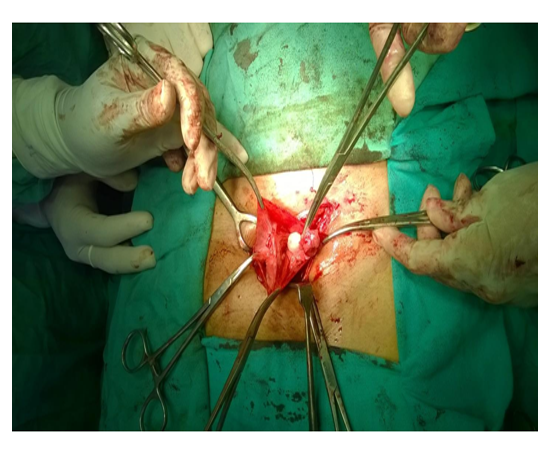
Figure2 .Left inguinal hernia with ovary as it content
3.Discussion
Inguinal hernias occur rarely in females around less than 5% of women. The diagnosis of an inguinal hernia can be made based on history and physical examination alone in the majority of cases. Inguinal hernias may present as an asymptomatic finding such as a painless bulge in the groin, with mild to severe abdominal-pelvic pain. Inguinal hernias in female must be promptly evaluated due to possible strangulation of organs, including, on rare occasion, the ovary and fallopian tube. Entrapment of adnexa in an indirect inguinal hernia is rare in adult women. Most of the cases which were reported were mainly seen in pediatric age group in whom ovaries and tubal herniation as unusual contents.
The reported incidence of its occurrence is 71% in children under 5 years and 30% in adolescents or women in reproductive age group and 2.9% exclusively in elderly females. At around 6 weeks of intrauterine life parietal peritoneum evaginates as processus vaginalis. The female counterpart of processus vaginalis usually disappears by 8 months of intrauterine life but may sometime persist as the canal of nuck. This persistence may be attributed to the hydrocele of the canal of nuck or inguinal hernia. One of the published reports laid the hypothesis that if there is failure of the fusion of the Mullerian ducts leading to the excessive mobility of the ovaries and non fusion of the uterine cornuae, the chance of herniation of the ovary into the inguinal canal is increased. Reports have been documented of herniation of not only the ovary but fallopian tube and even the herniation of the entire uterus into the inguinal canal of female infants. Researchers have documented that when the ovary is herniated completely, only the fallopian tube is attached to the ligament in the sac and ovary and its vessels do not adhere to the sac itself. In cases when uterus also herniates, the herniated part of the uterus also adheres to the sac and needs a careful exploration. In our case it was sliding inguinal hernia with ovary as it content, which could be due to a long ovarian ligament and broad ovarian mesentery. The sac should be opened in the normal appearing portion, and the walls inspected for a sliding component. The mesenteric attachment of the inner sac wall is divided in the bloodless plane within the sac. The freed up tube and the ovary is then reduced easily with no compromise in the blood supply and the neck of the sac is closed in the usual way. Since the tubes were not present in the sac, we were able to reduce the ovaries easily intra peritoneally and excised the sac after ligation at neck.
Immediate operation should be done in all patients who are ill with obstructed or locally inflamed hernia, without attempting reduction.
4. Conclusion
Inguinal hernia occurs rarely in females. The possibility sliding hernias containing genital structures such as ovaries, fallopian tubes or even the uterus should be kept in the mind in all female hernia and should be evaluated carefully in order to ensure proper surgical intervention in a timely fashion in order to prevent and relieve torsion and to return normal perfusion to the adnexa when the contents are adnexa. Multiple imaging studies may be necessary to assistin diagnosis, including ultrasound and/or cross-sectional imaging by computed tomography (CT), if a clinical suspicion is made preoperatively.
References
- Chawla S. Inguinal hernia in females. Med J Armed Forces India 2001;57:306-8.
- Gurer A, Ozdogan M, Ozlem N, Yildirim A, Kulacoglu H, Aydin R. Uncommon Content in Groin her-nia Sac. Hernia. 2006; 10: 152-5. [Pubmed].
- E. Kark and M. Kurzer, "Groin hernias in women," Hernia, vol. 12, no. 3, pp. 267–270, 2008.
- V. M. J. Sherman and F. C. Brunicardi, "Inguinal hernias," in Schwartz's Principles of Surgery, McGraw-Hill, New York, NY, USA, 9th edition, 2010.
- Gurudutt Bhaskar Basrur , Bilateral Inguinal Hernias Containing Ovaries , Clin Pract. 2015 Jan 28; 5(1): 708.Published online 2015 Mar 30.
- P. Kapur, M. G. Caty, and P. L. Glick, "Pediatric hernias and hydroceles," Pediatric Clinics of North America, vol. 45, no. 4, pp. 773–789, 1998