


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Proximal and Distal Rupture of the Biceps of the Arm in Athletes
Benigno Zenteno, M.D
Copyright : © 2016 Benigno Z. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Summary
Objectives: To help becomefamiliar to all Sports Professionals with this type of injuries in athletes. Remarking the difficulty to realize the clinical and imaging diagnosis. Emphasizing arthroscopy as an essential tool for the diagnosis in proximal lesions. And to offer the current modalities of management and in the distal injury to suggest one incision and the utilization of biodegradable material as fixation devices.
Conclusions: The injuries of the biceps tendon are primarily diagnosed with clinical and auxiliary imaging devices, but it is often necessary the arthroscopic corroboration in proximal lesions. The current techniques for fixation of the long head are various, but alike the distal injuries, the early fixation with biodegradable screws give an option biomechanically stable and promote the integral rehabilitation of the athlete.
Keywords: Biceps, Tendon Injuries, Athletes.
1.Introduction
One of the more important and disturbing questions of an athlete with a biceps injured is: what is the percentage of the tear?And what will be the deficiency if I do not have a surgical reconstruction?.The answer to these questions by the treating physician is controversial and imprecise includingthose using sophisticated imaging studies. (1, 2, 7, 10, 11, 14, 18, and 19). An adequate arthroscopic inspection of the affected shoulder, is one of the more important steps for the diagnosis and treatment of chronic tendinitis in the proximal insertion of the biceps tendon, which can evolve to a partial rupture, or the absence of the insertion of the long head in the glenoid.(2, 10, and 15).
At the other end of the extremity, the distal tendon rupture of the biceps is an uncommon reported lesion, but there is a general consensus that it will leave sequel in the sports practitioner if it is not managed surgically (4,5, 16). Avoiding this kind of reconstructionsby some surgeons for their potential complications reportedpreviously in the literature (9, 12, 16, 19).
The objective of these case presentations is to provide a clear idea of the usefulness of arthroscopy for the proximal injury in athletes, as a diagnostic and therapeutic tool, and at the same time the current modalities in their management. Related to the distal pathology,to offer a simple and effective approach for the sports people with this lesion. And concluding that if they are treated adequately, the athletes can return to their sports at the same level before their injuries.
2.Case 1
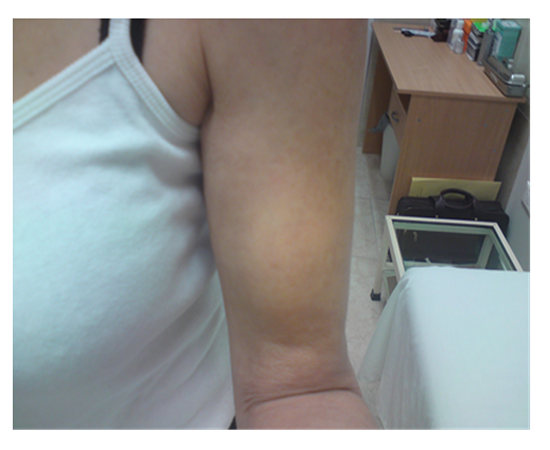
A 38 yearmale tennis player and weight lifter, felt a "cracking" in his right dominant shoulder, with no previous pain at all, this event occurred after weight lifting in the "preacher" bench curl. After that, he noticed a difference in volume of his arms (Figure. 1). At office consultation an imprecise ultrasound diagnosis was presented, and we decided to realize and arthroscopic procedure, where we found a complete rupture of the long head of the biceps reflected by an absence of the insertion of the tendon in the glenoid (Figure. 2).
Figure1. 38 Years Tennis Player

Figure 2. Arthroscopic Findings
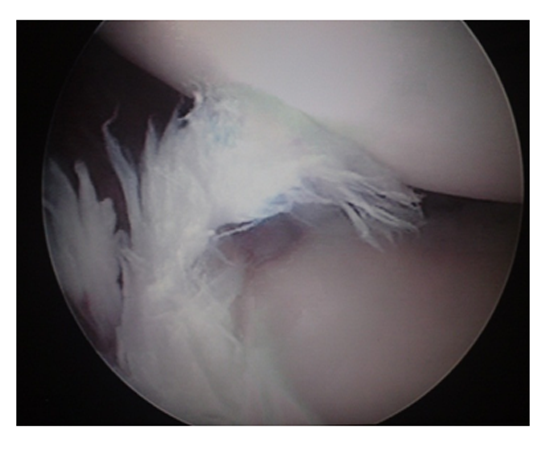
Figure 3. Surgical Findings. Subpectoral Approach
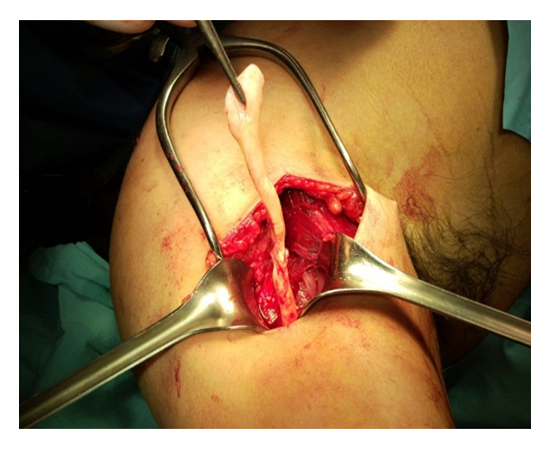
Figure 4. Fixation with Biodegradable screw
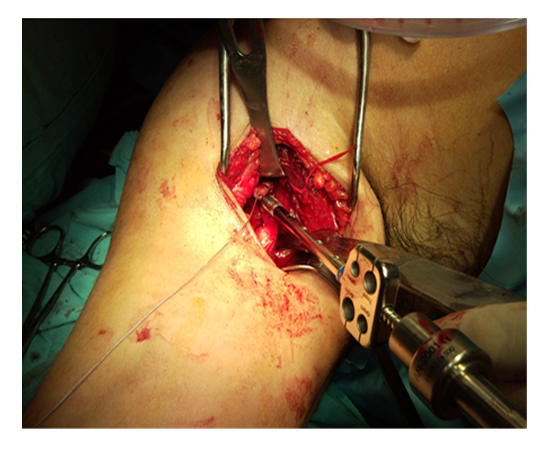
Figure 5. 2.8 Years after the Surgery. Playing Tennis and Lifting Weights

3.Case 2
A 60 year old right handed swimmer, with an average swimming of 2 Km. 4 times a week during 40 years, started with pain in the left shoulder 1 year before consultation. Three months before her office appointment the pain was presentduring all day and required constant analgesic administration. She noticed a "deformation" of the arm (Figure. 6), limitation of the arc of motion and crepitation during abduction.
Figure 6. A 60 Year Old swimmer, Long Head Biceps Rupture
At physical examination we found pain in the ventral portion of the left shoulder, corresponding to the intertubercular groove of the humerus, positive "Popeye" and Speed signs, and negative "bear hug sign" (10, 11). The MRI reported: Injuries of the subscapular and long head of the biceps, without mentioning the supraspinatus tendon.
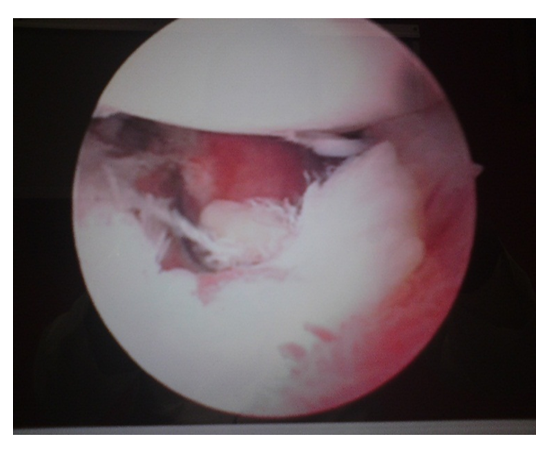
At arthroscopy the findings were: Partial rupture of the subscapular tendon, and a complete rupture of the long head of the biceps at the glenoid insertion (Figure. 7). In the sub acromial space, a complete rupture of the supraspinatus tendon was found.
Figure 7. Arthroscopic Findings of the Female Swimmer
A sub acromialarthroplasty was performed for a grade III acromion. And a biotenodesis of the long head of the biceps was performed with a biodegradable screw at the intertubercular groove level of the proximal humerus. The supraspinatus tendon was repaired with a "mini-open" incision with two metal anchors.2.6 years after the surgery she is swimming again at the same level previous to her ailments (Figure 8). UCLA classification: 33 points
Figure 8. 2.6 Years after the Surgery

4.Case 3
A 48 year, Male boxer and "weight lifter", presented with a history of been fighting and when he hit the contrary on his pelvis, felt a sudden pain in his left arm, followed by edema and ecchymosisin the elbow (Figure. 9). After a sonographic examination a "partial injury of the biceps" was reported in the "musculo-tendinous" portion.
Figure 9. 48 Year Boxer with a Complete Distal Biceps Rupture. Left Arm

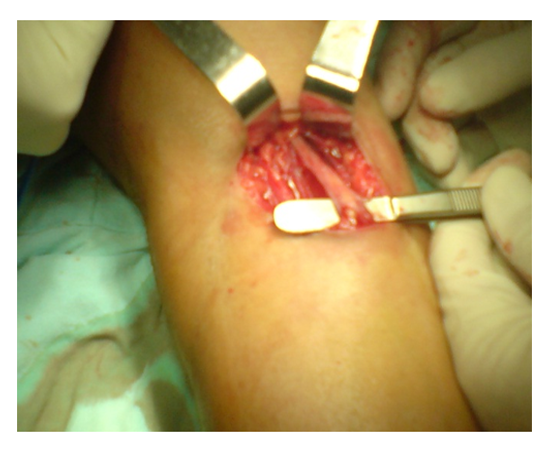
At the operating room, a complete rupture of the distal biceps tendon was found, with integrity of the aponeurotic expansion (Figure. 10). A repair of the tendon to the radial tuberosity was done with a biotenodesisbiodegradable screw, utilizing a single ventral incision.
Figure 10. Aponeurotic Expansion of the Biceps
The patient was reintegrated to all sports at 4 months after the surgery, including boxing.
Two years after the surgery he presented a new complaint but this time in the right arm, and clinically and arthroscopically a complete rupture of the proximal portion of the right biceps was diagnosed, and fixed subpectorally with a biodegradable biotenodesisscrew .
After 3 years of the surgerieshe is doing well in all his athletic performances, including "crossfit"(Figure. 11 and 12). And was classified with anUCLA score of 35 points of the right shoulder.
Figure 11. Distal Left Biceps 3 Years after the Surgery Left Arm

Figure 12. Same Patient in Figure 11 with the Right. Proximal Biceps tendon repaired with subpectoral technique. Years after the surgery.

5.Discussion
The complaints of the "shoulder" are common in athletes that use frequently the arms for their respective sports. This broad anatomic area is full of pathologic conditions, which etiology is in the majority of cases an "abuse" of the joints, with the development of "fatigue" and the loss of the appropriate biomechanics of the long head of the biceps which acts as a depressor of the humeral head and alsobeing primordial in the acceleration and deceleration movements of the arm. (3, 6).
The correct diagnosis is not easy to realize, mainly in partial injuries where the false negatives studies are reported (21). The lesions located at the "entrance" of the intertubercular groove are difficult to diagnose including those studied with a "high resolution" MRI. (1, 7, 10, 11, 14, 18).
The only precise diagnostic tool for the ruptured long head of the biceps is the "arthroscope", but must be handled by "expert orthopedic arthroscopic surgeons" (10).
The surgeon must have enough dexterity and experience to inspect adequately the long head of the biceps including the extra-articular portion in the "entrance" at the intertubercular groove and be prepared during the same surgical procedure to handle any kind of injury, e.g. :tenotomy, biceps fixation to the humerus, including a sub pectoral incision if this is necessary, mentioning the literature this last option as the safest for athletes (2,3,6,17).
Talking about the distal biceps, the diagnosis is neither easy as in the proximal injury. Some authors recommend the Hook test, but we found it difficult to elicit in the acute injured athlete because of the presence of pain an edema in the area (22). We trusted more in the history of the patient, with an eccentric extension load applied to the elbow (16), pain in the injured area and the presence of ecchymosis at the forearm (Figure 9).Because of these positive clinicals signs we decide to take the patients to the operating room despite the diagnosis of "partial" tear made by the sonographic radiologic reports(19).
We found the trend from people attending athletes tosuggest "not repair these distallesions", maybe based on the uncommon of the injury and also thinking about the complications reported in the literature, e.g: the iatrogenic injury of the median and musculocutaneousnerves (9).
Nonetheless, no matter the controversial issues related to these problems of the distal biceps , the current approach in sports people is to repair as soon as possible these lesions in athletes, with an anatomic fixation, to offer the patient the maximum muscular strength, avoiding also a lack of flexion or supination in the future (4,8,12)
The utilization of biodegradable materials provides the athlete the advantage of enough biomechanic strength of the biotenodesis implant, without the disadvantages of the "metallic screws" or other kind of non-degradable materials. The current biodegradable screws allow the athlete to obtain an integral rehabilitation because of the early mobilization of the injured arm. (5, 19).
In conclusion if we diagnose and treat adequately these athletes we can return them to their previous levels in their sports with minimum morbidity and these results are maintained in the long term follow up.
References
- Armstrong A, Teefey SA, Wu T, et al: The efficacy of ultrasond in the diagnosis of long head of the bíceps tendon pathology. J Shoulder Elbow Surg. 2006; 15 (1): 7-11.
- Busconi BB, De Angelis N, Guerrero PE: The prximal biceps tendon: tricks and pearls. Sports Med Arthrosc. 2008; 16 (3):187-94.
- Eakin C, Faber K, Hawkins R, eta al: Biceps Tendon Disorders in Athletes.J Am AcadOrthop Surg. 1999; 7(5): 300-10
- Chillemi C, Marinelli M, De Cupis V: Rupture of the distal biceps brachii tendon: conservative treatment versus anatomic reinsertion—clinical an radiological evaluation after 2 years. Arch Orthop Trauma Surg. 2007; 127 (8): 705-8.
- Fenton P, Quereshi F, Ali A, et al: Distal biceps tendon rupture. A new repair technique in 14 patients using the biotenodesis screw. Am J Sports Med. 2009; 37: 2009-2015.
- Fierdman DJ, Dunn JC, Higgins LD, eta al: Proximal biceps tendon: injuries and management. Sports Med Arthrosc. 2008; 16 (3):162-9.
- Gaskin CM, Anderson MW, Choudri A, et al: focal partial tears of the biceps brachii tendon at the entrance of the bicipital groove: MR findings, surgical correlation and clinical significance.Skeletal Radiol.2009: 38 (10): 959-65.
- George MS: Simultaneous acute rotator cuff tear and distal biceps rupture in a Strongman competitor. Orthopedics. 2010; 16 : 268-270.
- Gregory T, Roure P, Fontes D : Repair of distal biceps tendon rupture using a suture anchor. Am J Sports Med. 2009; 37 (3): 506-511.
- Gill H, El Rassi G, Bank M, et al: Physical examination for partial tears of the biceps tendon. Am J Sports Med. 2007; 35 (8):1334-40-
- Kibler W, Sciascia A, Hester P, et al: Clinical utility of traditional and new tests inthe diagnosis of biceps tendon injuries and superior labrum anterior and posteriors lesion in the shoulder. 2009; 37 (9): 1840-7.
- Kokkalis ZT, Sotereanos DG: Biceps tendon injuries in athletes. Hand Clin. 2009: 25 (3):347-57.
- Lyons RP, Green A: Subescapularis tendon tears. J Am AcadOrthop Surg. 2005; 13:350-363.
- Moosmayer S. Smith HJ: Diagnostic ultrasound of the shoulder—a method of experts only? Results from an orthopedic surgeon with relative inexpensive compared to operative findings. ActaOrthop. 2005; 76 (4): 503-8.
- Nho S, Strauss E, Lenart B, et al: Long head of the biceps tendinopathy: Diagnosis and mangement. J Am AcadOrthop Surg. 2010; 18: 645-656.
- Quach T, Jazayeri R, Sherman OH, et al: Distal biceps tendon injuries—current treatment options. Bull NYU HospJt Dis. 2010; 68(2): 103-11.
- Tangari M, Carbone S, Gallo M, et al: Long head of the bíceps tendon rupture in professional wrestlers: Treatment with a mini-open tenodesis. J Shoulder Elbow Surg. 2010 Sep 29. (Epub ahead of print).
- Theodoropoulos JS, Andreisek G, Harvey EJ, et al: Magnetic resonance imaging and magnetic resonance arthrography of the shoulder: dependece of the level of training of the performing radiologist for diagnostic accuracy. SkeletalRadiol. 2009 Oct 14 (E pub ahead of print).
- Zenteno B, Lozano J, Villalobos E, et al: Ruptura distal del tendón del bíceps braquial, tratamiento quirúrgico con una incisión y fijación con material biodegradable. Presentación de un caso y revisión de la literatura. Acta Medica Grupo Ángeles.2004; (4):247-50.
- www.orthopedicscores.com, May 12th, 2014.
- Hegedus EJ1, Goode AP, Cook CE,et al: Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with metaanalysis of individual tests. Br J Sports Med. 2012 Nov; 46(14):964-78.
- O'Driscoll SW1, Goncalves LB, Dietz P.:The hook test for distal biceps tendon avulsion.Am J Sports Med.2007 Nov;35(11):1865-9.