


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Knife Blade Penetrating as a Non Missile Injury to the Cervical Spine through the Face. A Case Report
Joseph Musowoya1, Duncan D Mugala2, Alick Mwambungu3, Womba Kadochi4, Nathan Siulapwa5
2.BSc, MB ChB, MMed (Surgery), FCS (ECSA).Senior Lecturer: Copper Belt University-School of Medicine, Zambia.
3.BSc, MSc (Haem) Senior Lecturer: Ndola College of Biomedical Sciences, Zambia.
4.BSc, MB ChB, Registrar General Surgery Ndola Central Hospital, Zambia.
5.BSc, MSc, PhD, Head Basic Sciences Copper Belt University- School of Medicine, Zambia.
Copyright : © 2016 Joseph M. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Spinal cord stab injuries (SCSI) are rare traumatic lesions when compared to injuries caused by road traffic accidents, sport activities and guns. We report a case of a 31-year-old male who was hospitalized because of being stabbed on the face and the blade penetrated the cervical spine. This was a serious physical violence between two men fighting over a woman. On admission, the patient had left hemiplegia with loss of reflexes and loss of sensation. All cranial nerves were intact, the heart sounds were normal though the patient was unable to shrug his left shoulder. The knife in our patient was very close to the vertebral arteries and the Circle of Willis. However, the long knife was gently removed and no significant bleeding or leakage of the cerebrospinal fluid occurred. The patient was put on antibiotics to avoid infections. The initial management of SCI is crucial for protecting undamaged spinal cord from secondary effects and Surgery should be considered as the first-line treatment in cases of incomplete injuries of the spinal cord with retained metallic object. In spite of scientific progresses, it is still not possible yet to repair a damaged spinal cord.
Keywords: Knife, Stab, Face, Spine, Paralysis, Cervical.
1.Introduction
Violence is a social disease that plagues all societies. Each society has its own form of violence. Chingola is a mining town in Zambia with a population of about 200,000 people. Chingola, like any other town has reports of violence and in the past, the pattern of physical violence in that town has been recorded [1]. The most frequently affected age group of violence in Chingola is in the range of 21 to 30 years.
In this town victims of physical violence come from all the townships of Chingola. However the majority of the victims come from the medium and high density areas and very few victims come from low density areas [1].
It has been established that the most violent place is the home and this accounts for about 53.1% of all violent cases reported. Despite the fact that the most violent attackers are the thieves, the next most common attacker is the husband and the wife is the lowest attacker [1] .
The most common cause of violence in a home is domestic confliction, where 85% of the women are the victims. The men (50%) are largely victims of thieves.
It is known that the men are the most Knifed or stabbed (rarely by the wife) and commonly by the thieves. Violence involving use of stones are also widely seen in men and less so in women. The majority of the injuries in Chingola occur in the domestic situations. It is clear that victims are more likely to get a serious injury in a domestic conflict than in criminal violence or other conflicts.
Authors are reporting on a case of a 31-year-old man who was stabbed on the face and the blade penetrated the cervical spine. This was a serious physical violence between two men fighting over a woman.
Spinal cord stab injuries (SCSI) are rare traumatic lesions when compared to injuries caused by road traffic accidents, sport activities and guns [2] . The disability resulting from spinal cord injuries (SCI) puts a heavy burden on victims and the whole society concerning quality of life, working time loss and financial cost [3]. Stab injury of the spinal cord is a rare occurrence and its incidence varies according to the country. In the United States, only 1% of the spinal cord injuries result from stabbing [4]. In a large series from South Africa, 25% of spinal cord injuries were reported to result from sharp injuries and 84.2% of these sharp injuries resulted from stabbing [5]. Most of the injuries are caused by hemi-section of the spinal cord that results in incomplete neurological deficits [5].
The initial management of SCI is crucial for protecting undamaged spinal cord from secondary insults. In spite of scientific progresses, it is still not possible yet to repair a damaged spinal cord.
2.Case Details
The victim was male, aged 31 years of age and lived in Mulando Township in Chingola, Zambia. He had separated from his wife with whom he had one male child who was 8 years old at the time of the incident. The victim was admitted to Ndola Central Hospital on 23rd October 2015 and was complaining of pain in the neck.
Circumstances surrounding his separation from his wife were that they had lived together for about 8 years prior to this incidence. He then left town and went to Lusaka to work for his uncle for about 6 months. When he came back, he found that his wife was living with another man with whom she was pregnant for .The family sat together and resolved that the relationship between the patient and the 'wife' separate; and allowed her to marry her new partner who was dealing in mineral stones and had more wealth
On Thursday 22nd October 2015, the patient went to visit his ex-wife at her home despite being separated.
While the patient and his ex-wife were sleeping in bed around 22:00hrs, he felt being hit on the face with a large object. He then woke up and noticed his ex-wife's new husband had stabbed his face with a knife and run out of the bedroom. His ex-wife and his parents rushed him to hospital from the moment he was injured, the patient had been unable to move his left upper and lower limbs.
3.Patient Examination
On examination the patient had left hemiplegia with loss of reflexes and loss of sensation. All cranial nerves were intact, the heart sounds were normal. Patient was unable to shrug his left shoulder.
Figure.1a and 1b shows knife blade embedded through the victim’s face
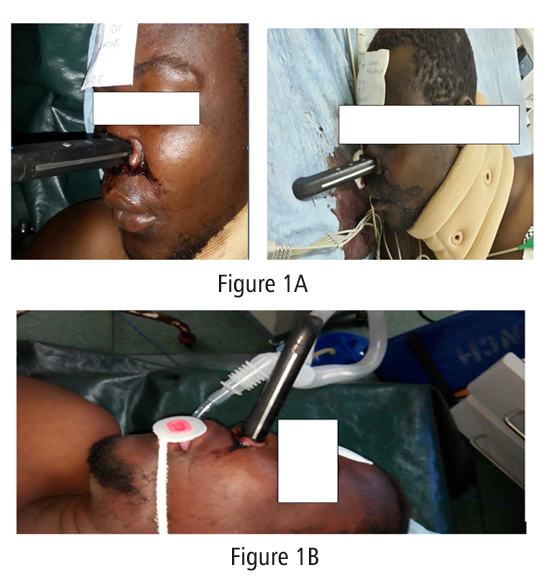
Figure 2. a and b shows the extent of knife blade penetration
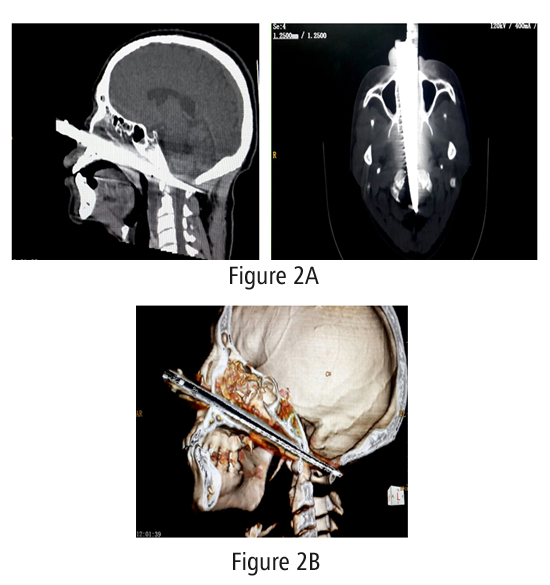
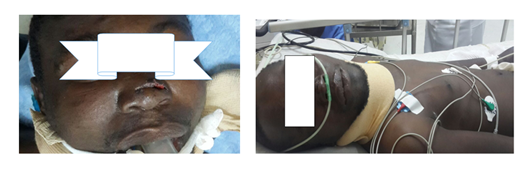
Figure 3. After removal of the knife

Figure 4.Knife used in the attack

Figure5. a and b shows the patient recuperating after removing the knife
4. Discussion
It is true that Knife related stabs cause more disabling injuries than any other types of hand tools [6]. The patient ended up with complete left hemiplegic (paralyzed from the upper limb to the lower limb). Knives represent an important source of morbidity and mortality to people in all ages.
Brain stab wounds usually also cause numerous complications like Intracranial hemorrhage, Injury of important vessels and infection. Minimal blade movements during removal and precautiousness to prevent massive hemorrhage is essential. Lwakura M et al [7] reported a 28 year old man who attempted to kill himself with a knife by stabing his brain. They had to take measures to prevent complications. In our patient we carried similar measure as we removed the Knife and made sure that he did not lose too much blood and start losing Cerebral Spinal Fluid (CSF).
Sweeney et al [8] reported that non missile penetrating injuries are uncommon wounds in modern times. Their cases showed knife injuries to the brain but without large hematomas'. This fact was also true in our patient. It was an unusual injury we have seen around in Chingola, Zambia. In their first case a 31 year old patient stabbed himself to the head through the neck arterioles covering the trachea in trying to kill himself. He was taken to theatre, a tracheotomy was made to secure the airway and the knife was removed. The anterior cranial fossa was repaired he was kept in ICU. He was discharged upon recovery with atracheostomy which was reversed after three months. He recovered well.
Our paper is a case report of two men who married one woman; the famous (three) love triangle. This was similar to Sweeney et al's second patient who in their case was a lady aged 21 years old. It was a woman in a three triangle love. She was stabbed though the eye. In her case, the stab went close to the Petrous Carotid and the Cerebral Arteries. The Patient underwent a Cranio-Orboto-Zygomatic approach to remove the knife to avoid the neuron- vasculature. The proscribed vascular control was obtained. In the ICU, respiration returned to normal. The repeat CT showed no hemorrhage later.
The Third patient was 24 year old who was stabbed with a screw driver and was confused at the time of attendance. A right frontal Craniotomy for a neurocysm reconstruction and exploration of the Injury bed was done. He recovered well.
In all the cases of non missile brain penetration, a CT scan is highly essential and an effective tool for initial investigation of penetration of the brain. However, it must be said that brain injuries where there is plastics, wood or soil, the CT may not yield much. A CT is also highly essential for the Angiogram in brain injuries. The Craniotomy should by and large, be done but in our case we could not do one because the injury was the base and the trajectory of the impaled knife was nearly in accessible but did cause potentially fatal damage. We feared the Willis circle being injured, but the patient survived well.
Muhomeed et al (9) shows that Trans-orbital penetrating injuries are uncommon but may cause brain injuries. Their case was a man of 59 years old who was feared could lose his eye. He had complete Ptosis with some ecchymosis. The knife was close to internal carotid artery. In our case the knife in our patient was very close to the vertebral arteries and the Circle of Willis. They had no CT but we had a CT although we could not do angiography. We could just imagine how close the patient's vessels were. The Knife in their patient was gently removed and the patient never bled as feared and the eye recovered well. We too had to gently remove the long knife and we had no significant bleeding or leakage of the cerebrospinal fluid.
Sosuncu et al (10) showed that some brain injuries may result from small stabs which may be difficult to see and a CT scan or X Ray may show only a small puncture injury. In our case the inflicting object used was a large Knife.
Cranio cerebral injuries penetrating the brain are not common. Worse still if they remain impaled for a long time. In these cases of prolonged impalement, it is worrisome to the operators wishing to remove them for fear of foreign body adherence to the nervous tissue and a higher risk of further injury is expected from removal. In our patient there was long stay. We however, did not expect these risks. Our fear was bleeding and CSF leakage. Dias Filho Et al [11] performed a craniotomy and carried out their removal of a three year brain Knife using meticulous approach with minimal dissection and minimal oscillation of the blade thus avoiding damage to the adjacent structures. There were no complications in their patient.
In our patient, no expected complications occurred and there were no infections. The patient was put on antibiotics prophylactically. Of all the reports reviewed, we did not come across presentation with neurological sequelae. Our patient presented with primary paralysis of the entire left side of the body below the injury; he was hemiplegic.
We are hoping the patient may recover after three months. If not it may be a permanent paralysis.
In a few and rare case there has been some patients who have self injured themselves with no initial of self inflicting themselves but in the process of using the knife they have stabbed themselves. Hirt M, and Karger B, [12] report a case of fatal brain injury caused by free flying of a Knife which was being used by the person on his business and the flying knife entered his brain, perforating the Orbital cavity and the frontal lobe on the right side and the patient died. In our case it was an infliction by the second husband. Our patient did not die and he survived.
It is worthy to note that, not all patients who undergo Knife brain injuries survive some have died. Our patient who was aimed at being killed him survived. Fukube S et al [13] carried out a retrospective study which showed that in a period from 1995 to 2095 a percentage of 2.5% of the patients died. It showed that more males than women died from these injuries. The majority of those who died were in the age range of 50 to 70 years. Our patient though was meant to be killed survived. It is of interest to note that in this study of all the injuries causing death there was no death arising from Knife brain injuries causing death. This shows that brain injuries are rare.
5. Conclusion
Knife blade penetrating as a non missile injury to the cervical spine through the face which is part of the head are not common. Even in Chingola, it is a case that has not been recorded before hence very rare. The causes are usually as a result of trying to kill themselves or injuries arising as a result of work. Quiet frequently these injuries are often the result of the three triangle love affair. Our patient was the involvement of the love triangle affair. Despite this trauma he did not die but he has become paralyzed in the left upper and lower limbs. It is hoped that he will eventually recover and resume walking.
References
- Duncan D Mugala, Doreen Imataa:Admisions for physical violence in Chingola –Zambia, East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 68-73
- Yeung, J. and Karim, A. (2012) Complete Spinal Cord Transection from a Stab Wound with Surgical Precision. Journal of Emergencies, Trauma, and Shock, 5, 204.
- Wyndaele, M. and Wyndaele, J.J. (2006) Incidence, Prevalence and Epidemiology of Spinal Cord Injury: What Learns a Worldwide Literature Survey? Spinal Cord, 44, 523-528.
- Burney RE, Maio RF, Maynard F, Karunas R: Incidence, characteristics, and outcome of spinal cord injury at trauma centers in North America. Arch Surg 128: 596-609, 1993
- Peacock WJ, Shrosbree RD, Key AG: A review of 450 stabs wounds of the spinal cord. S Afr Med J 51: 961-964, 1977
- G A Smith, Knife related injuies treated In the U S Emergency department. Journal of Emergency Med: 2013 Sept.43 (3)315-23
- LwakuraM, KawagutiT,Husada K, Shibata Y, KumatsuH, Yonakisowa A, Kohimara E. Knife blade pernatrating stab wounds to the brain. A case Report: Neuro Med Chir(Tokyo) 2005 Mar,45(3) 172-5
- Sweeney JM,LebovitzJ,EllerJL,CoppensJR,Bucholz RD, Abudulrouf SI ; Management of non missile penetrating brain injuries –A description of three cases and review of literature:Skull Base reports 2011May,1(1)39-46.
- Muhomeed A, Rehmen A,WaleedT, Alebredy, Basim H,Akhils K; TransorbitalStab injury with a retained Knife; A normal escape: A case report. A Case Report in Critical care Vol 2014 (2014) articleID754053, 5
- Sosuncu E, Hakan A, Ismail G, Yarden A, Mehet A: Concealed Penetrating parietal lobe injury due to stab wound, A case Report. Austin J. Emergency and Critical Med. 2014; 1(1)2
- Dias Filho LC, de Borros AC, da Mata MF, Three years with a knife stuck in the brain; Faculty of Medicine Pernambuko Federal University Recife PE Brazil.
- Hirt M, Karger B. Fatal brain injury caused by free flying of a Knife a case report and evaluation of the unusual weapon: Internationaljuornal of legal Medicine. August 1999, Volume112 issue5, pp313-315.
- Fukube S, Hayashi T, Kondo T; Retrospective Study on suicidal cases by sharp force injuries ; Journal of Forensic and legal Medicine April 2008, Volume 15 (3):163-167.