


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
The Role of Cardiac Computed Tomography in the Diagnosis of Takotsubo Syndrome: Short Review with a Demonstration of a Case
Shams Y-Hassan,Elin B Brolin
2.Department of Radiology, Sweden.
Copyright : © 2017 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Takotsubo syndrome (TS) and acute coronary syndrome (ACS) have identical clinical and electrocardiographic presentation. Invasive coronary angiography (CAG) and left ventriculography are decisive in distinguishing the two conditions. However, in the presence of life threatening co-morbid conditions such as terminal malignancy, patient age and frailty, invasive CAG may imply substantial increase in the risk of complications. In some other patients where the likelihood of obstructive coronary artery disease is minimal, invasive CAG with its associated risks may be unnecessary. In addition, some other patients may have bad echocardiographic acoustic windows or contraindications to cardiac magnetic resonance imaging. In such circumstances, non-invasive cardiac computed tomography (CT) may be the appropriate diagnostic alternative with the ability to provide information on both the coronary arteries and the left ventricular wall motion abnormality. Herein, we discuss the role of cardiac CT in the diagnosis of TS illustrated in a case of 53-year-old woman with mid-ventricular pattern of TS, myocardial bridging of left anterior descending artery and otherwise normal coronary arteries detected by cardiac CT.
Takotsubo; computed tomography; broken heart syndrome; apical ballooning; acute coronary syndrome,Cardiology
1. Introduction
Takotsubo syndrome (TS) is an acute cardiac disease entity with a clinical and electrocardiographic presentation resembling that of acute coronary syndrome (ACS)[1,2]. The disease is affecting predominantly women and characterized by a unique circumferential typically regional left ventricular wall motion abnormality (LVWMA) resulting in a conspicuous left ventricular ballooning during systole [1-3]. The ballooning pattern of the left ventricle may be localized to the apical, mid-apical, mid-ventricular, mid-basal, and basal regions of the left ventricle; focal and global patterns, and the right ventricular involvement have also been reported [4-6]. The term Takotsubo was introduced in 1990 to describe the silhouette of the left ventricle during systole, which resembles a Japanese Octopus pot, in patients presented with a clinical picture of myocardial infarction with no obstructive coronary artery disease [7,8]. Because of the identical clinical presentation of TS and ACS,the most important point in the differentiation of the two conditions is to disclose the coronary anatomy and the LVWMA pattern. This can be achieved by invasive coronary angiography (CAG) with the advantage of performing coronary intervention if an acute coronary culprit lesion is detected especially in patients with ST-elevation myocardial infarction (STEMI) like electrocardiographic (ECG) changes. However, under certain circumstances, non-invasive cardiac computed tomography (CT) can be utilized for the same diagnostic purposes avoiding the risks of invasive CAG. Herein; a case of mid-ventricular TS diagnosed by non-invasive cardiac CT is described. A proposal for the most appropriate indications for cardiac CT in TS diagnosis with a short review is provided.
2. Case Presentation
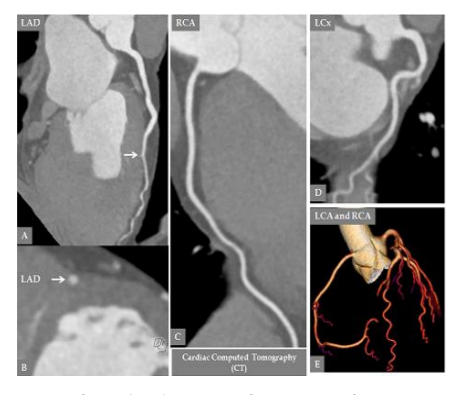
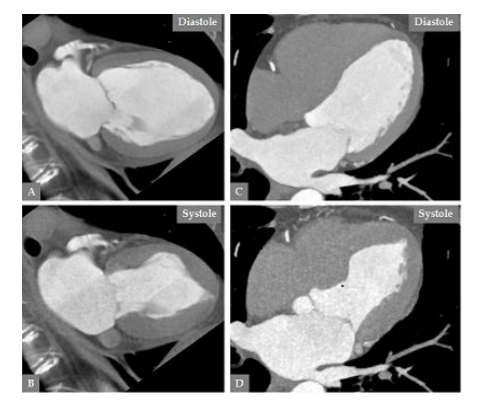
A 53-year-old woman presented with dizziness, syncope and head injury. The patient was medicated for chronic anxiety and depression with Sertraline and Agomelatine (Valdoxan). She was a chronic smoker (4-5 cig/day). The patient had no history of diabetes mellitus or epilepsy. On the day of presentation, the patient was under mental stress and visited a psychiatrist for panic disorder and depression. A few hours later while being in a market, she experienced dizziness followed by syncope that led to head injury with swelling at the occipital region of the head. Witnesses observed that the patient was shaking. She had not bitten her tongue. At the emergency department, the patient did not have chest pain. She was well-oriented with normal pulse and blood pressure. Clinical examination and auscultation of the heart, lungs and abdomen were normal. The neurological examination was completely normal. Emergency CT of the brain showed no evidence of intracranial bleeding or cerebral infarction. Blood glucose was normal (5.8mol/L). There was mild elevation of high sensitivity troponin T (152nanog/L). Furthermore, review of the patient`s history revealed that she had probably experienced mild chest discomfort before and after the syncope attack. Because of the basically normal electrocardiogram, the absence of real chest pain and the very mild elevation of troponin T levels, the likelihood of finding obstructive coronary artery disease was deemed to be minimal. Thus, the patient was referred for non-invasive cardiac CT. Cardiac CT data acquisition was performed on a dual source 2x64-row CT scanner, using a dose-modulated retrospectively ECG-triggered scan protocol. Interactive image processing software was used for CT data analysis. The examination revealed normal coronary arteries apart from a short segment of the left anterior descending artery (LAD) with myocardial bridging (Fig1. A, B, C, D and E). In order to assess the LVWMA, multiphase datasets were reconstructed at 5 % increments of the RR interval (0-95%) and 4-mm-thick multiplanar reformatted images were reconstructed, in standard cardiac planes. Evaluation showed circumferential hypokinesia/ akinesia of the middle segments of the left ventricle with normal/ hypercontraction of the apical and the basal segments resulting in a conspicuous ballooning of the left ventricle (FIG2. A, B, C, and D). These findings were consistent with the diagnosis of mid-ventricular pattern of TS. Right ventricular function was not assessed, since the contrast agent concentration in the right ventricle was insufficient to allow for reliable delineation of the ventricle. Echocardiography a few hours later confirmed the findings of cardiac CT, with mid-ventricular ballooning and estimated ejection fraction 53%. The patient discharged herself one day after admission on her own accord. Cardiac magnetic resonance imaging 3 months after the index presentation showed normal left ventricular contractility with normal EF 59%; there was no sign of myocardial infarction.
3. Discussion
TS and ACS have identical clinical and electrocardiographic presentation [2]. Invasive CAG and left ventriculography are crucial to differentiate the two conditions and with the benefit of the possibility of coronary intervention once detecting a coronary culprit lesion explaining the whole LVWMA. However, invasive CAG in certain patients with acute severe medical or surgical illness (as sepsis, acute intracranial processes), which may trigger TS, implies substantial increase in the risk of complications. In a recent study by Murugiah et al [9], a large proportion of patients were being coded with secondary diagnosis of TS who did not undergo CAG. The reasons for not performing coronary angiography are unknown but likely include the presence of life-threatening co-morbid conditions such as terminal malignancy, patient age and frailty. In such conditions, non-invasive cardiac CT may be an appropriate alternative to invasive CAG.
Furthermore, in patients with bad echocardiographic acoustic windows and in patients with contraindications to cardiac magnetic resonance imaging, cardiac CT, with the ability to provide information on both coronary anatomy and LVWMA, may also be considered. There are only a few publications in the form of case reports or images in cardiology using cardiac CT [10-14] in the acute setting of TS. Hara et al [10] in 2007 used multidetector row computed tomography to exclude significant coronary artery disease and visualize apical ballooning of the left ventricle in a patient with TS. The technique is frequently used to rule out acute aortic diseases, pulmonary embolism and high-grade coronary stenoses in patients with acute chest pain. Scheffel et al [11] in 2008 could exclude pulmonary embolism in a patient with history of pulmonary embolism and meanwhile demonstrate signs of left ventricular mid-apical ballooning in the patient who had acute TS.
Matsuzono et al [15] in 2013 reported on a patient with TS complicated by cerebral embolic stroke. Coronary CT in that patient showed no coronary stenosis and contrast cardiac CT demonstrated hypokinesis of the apex with a 3-cm immobile thrombus. We have recently reported on a case of simultaneous an obtuse-marginal spontaneous coronary artery dissection (SCAD) and mid-apical pattern of TS [16]. Cardiac CT few days after admission could detect both recurrence of SCAD in the proximal part of the right coronary artery and the mid-apical pattern of TS. The cardiac CT may provide information on LVWMA when information is acquired throughout the cardiac cycle but this implies higher radiation exposure. In patients with suspected recurrent TS, cardiac CT may be an appropriate diagnostic alternative. Maroules et al [12] in 2009 could show normal coronary arteries and visualize mid-apical left ventricular ballooning with cardiac CT in a patient with recurrent TS. In the present case where the patient had no chest pain and the ECG was normal, the cardiac CT provided sufficient information about the coronary arteries and the diagnosis of TS, thus avoiding the risks of invasive CAG. The cardiac CT showed a short segment of the LAD with myocardial bridging, which could not explain the mid-ventricular LVWMA and normal apical contractions of the left ventricle [17]. Other investigators have also proposed cardiac CT as a noninvasive imaging modality alternative to invasive CAG to exclude coronary culprit lesions in patients with non-ST-elevation myocardial infarction like ECG changes and a clear clinical, as an elderly woman with an emotional trigger factor, and echocardiographic picture of TS, as circumferential mid-apical pattern with distal LAD flow visualization [18].
Consequently, non-invasive cardiac CT could be utilized as an appropriate diagnostic tool instead of invasive CAG in the following circumstances: 1) when the suspicion of acute coronary syndrome is low as in the current case or the patient refuses invasive diagnostic assessment; 2) in suspected recurrent TS; 3) in patients with elevation of myocardial infarction biomarkers during acute critical illnesses such as sepsis, intracranial diseases (e.g subarachnoid hemorrhage, ischemic stroke) and other critical conditions that may be complicated by TS; 4) in patients with bad echocardiographic acoustic windows and contraindications to CMR imaging; and in 5) patients with delayed presentation after an episode of chest pain or for a retrospective evaluation of a patient with the typical history of TS weeks before.
4. Highlights
1. The Role of Cardiac Computed Tomography in the Diagnosis of Takotsubo Syndrome (TS) is described.
2. A case of midventricular TS detected by cardiac computed tomography (CT) is presented
3. Non-invasive cardiac CT may be an attractive alternative for invasive coronary angiography for the diagnosis of TS in patients with severe chronic co-morbidities.
4. Other indications of cardiac CT in the diagnosis of TS are described as advanced age and frailty, terminal malignancy where invasive coronary angiography may be associated with substantial risks.
References
- Y-Hassan S, Acute cardiac sympathetic disruption in the pathogenesis of the takotsubo syndrome: a systematic review of the literature to date. Cardiovascular revascularization medicine : including molecular interventions 2014;15:35-42.
- Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. Journal of the American College of Cardiology 2010;55:333-341.
- Y-Hassan S, Clinical Features and Outcome of Pheochromocytoma-Induced Takotsubo Syndrome: Analysis of 80 Published Cases. The American journal of cardiology 2016;117:1836-1844.
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA, Seifert B, Hellermann J, Schwyzer M, Eisenhardt K, Jenewein J, Franke J, Katus HA, Burgdorf C, Schunkert H, Moeller C, Thiele H, Bauersachs J, Tschope C, Schultheiss HP, Laney CA, Rajan L, Michels G, Pfister R, Ukena C, Bohm M, Erbel R, Cuneo A, Kuck KH, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun-Dullaeus RC, Cuculi F, Banning A, Fischer TA, Vasankari T, Airaksinen KE, Fijalkowski M, Rynkiewicz A, Pawlak M, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Franz WM, Empen K, Felix SB, Delmas C, Lairez O, Erne P, Bax JJ, Ford I, Ruschitzka F, Prasad A, Luscher TF. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. The New England journal of medicine 2015;373:929-938.
- Y-Hassan S, Tornvall P, Tornerud M, Henareh L. Capecitabine caused cardiogenic shock through induction of global Takotsubo syndrome. Cardiovascular revascularization medicine : including molecular interventions 2013;14:57-61.
- Win CM, Pathak A, Guglin M. Not takotsubo: a different form of stress-induced cardiomyopathy--a case series. Congestive heart failure 2011;17:38-41.
- Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. [Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases]. Journal of cardiology 1991;21:203-214.
- Y-Hassan S, Yamasaki K. History of takotsubo syndrome: is the syndrome really described as a disease entity first in 1990? Some inaccuracies. International journal of cardiology 2013;166:736-737.
- Murugiah K, Wang Y, Desai NR, Spatz ES, Nuti SV, Dreyer RP, Krumholz HM. Trends in Short- and Long-Term Outcomes for Takotsubo Cardiomyopathy Among Medicare Fee-for-Service Beneficiaries, 2007 to 2012. JACC Heart failure 2015.
- Hara T, Hayashi T, Izawa I, Kajiya T. Noninvasive detection of Takotsubo [corrected] cardiomyopathy using multi-detector row computed tomography. International heart journal 2007;48:773-778.
- Scheffel H, Stolzmann P, Karlo C, Trigo-Trindade P, Marincek B, Luescher TF, Alkadhi H. Tako-tsubo phenomenon: dual-source computed tomography and conventional coronary angiography. Cardiovascular and interventional radiology 2008;31:226-227.
- Maroules CD, Linz NA, Boswell GE. Recurrent Takotsubo cardiomyopathy. Journal of cardiovascular computed tomography 2009;3:187-189.
- Nance JW, Schoepf UJ, Ramos-Duran L. Tako-tsubo cardiomyopathy: findings on cardiac CT and coronary catheterisation. Heart 2010;96:406-407.
- Otalvaro L, Zambrano JP, Fishman JE. Takotsubo cardiomyopathy: utility of cardiac computed tomography angiography for acute diagnosis. Journal of thoracic imaging 2011;26:W83-85.
- Matsuzono K, Ikeda Y, Deguchi S, Yamashita T, Kurata T, Deguchi K, Abe K. Cerebral embolic stroke after disappearing takotsubo cardiomyopathy. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association 2013;22:e682-683.
- Y-Hassan S, Themudo R, Maret E. Spontaneous coronary artery dissection and takotsubo syndrome: The chicken or the egg causality dilemma. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions 2017.
- Brolin EB, Brismar TB, Collste O, Y-Hassan S, Henareh L, Tornvall P, Cederlund K. Prevalence of Myocardial Bridging in Patients With Myocardial Infarction and Nonobstructe Coronary Arteries. The American journal of cardiology 2015;116:1833-1839.
- Citro R, Pontone G, Pace L, Zito C, Silverio A, Bossone E, Piscione F. Contemporary Imaging in Takotsubo Syndrome. Heart failure clinics 2016;12:559-575.