


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
ARC Journal of Anesthesiology
Volume-3 Issue-4, 2018, Page No: 1-2
Unexpected Danger: Obstruction of Endotracheal Tube by Tegaderm
Ebru Tarikci Kilic1*, Mehmet Salim Akdemir1, Egemen Atag1
1.Ümraniye Training and Research Hospital, Anesthesiology Department.
Citation : Ebru Tarikci Kilic, Mehmet Salim Akdemir, Egemen Atag, "Unexpected Danger: Obstruction of Endotracheal Tube by Tegaderm" ARC Journal of Anesthesiology. 2018; 3(4) : 1-2.
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
To The Editor
Iatrogenic airway obstruction by foreign body, clot plugs have been documented recently very well, I am compelled to report an unusual case of a complete airway obstruction by Tegaderm. We ndecided to share and to write our experience.
A healty ASA physical status class I,three years old 18 kg boy presented for External Ventriculer Drainage (EVD)insertion due to theintracranial hemorrhage. After induction of anesthesia 4.5 oral endotracheal tube (ETT)wassecured to the boy’s chin with plastic tape and Tegaderm dressing. We checked the ETT connections, then the patient was prepped and draped. The flow sensor alarmed low flow 10 minutes later. Tidal volume decreased. To solve the cause of low flow alarm we firstly expected the anesthesia ventilator, the connectionsof oxygen intake and the circuit of anesthesia. There was a leak in the system. We disconnect and reconnected the ETT. After reconnection, the ventilation didn’t improve. Tidal volume dropped immediately to 0 ml. We removed the surgical drapes to examine the patient. The patient was in cyanosis with no chest rise. We removed the ETT immediately, rapidly intubated again. After ventilating with 100% oxygen, oxygen saturation increased to 99%. We didn’t suspect broncospasm or laryngospasm. The patient was reprepared and surgery proceeded uneventfully. The postoperative period was unremarkable.
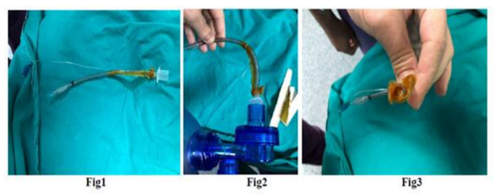
What we saw then the tegaderm in the ETT causing the obstruction internally in the distal end of the ETT by migration.
There are several acute management steps to consider when assessing the deterioration of oxygenation for an intubated patient. First tube occlusion must be considered. Occlusion of the endotracheal tube is very serious and life threatening event. Manuel ventilation should be the first , removing of the tube should be the second attempt in case of impossible suction. When it is not possible to remove the obstruction quickly, rapid reintubation must be performed [1,2].
There have been case reports which have been shown various tecniques in dealing with blood clot impaction in the ETT. Once obstruction is suspected, nearly all reports indicated a common algorithm for the management of the obstructed ETT. More importantly this rapidly results in life threating ventilatory problems.
In conclusion we present a patient who became hypoxic severely during the surgery due to the occlusion. Weare unaware of any similar case as ours, causing obstruction of the airway. Without any panic we overcame this serious complication which could have a fatal consequence.
Iatrogenic airway obstruction by foreign body, clot plugs have been documented recently very well, I am compelled to report an unusual case of a complete airway obstruction by Tegaderm. We ndecided to share and to write our experience.
A healty ASA physical status class I,three years old 18 kg boy presented for External Ventriculer Drainage (EVD)insertion due to theintracranial hemorrhage. After induction of anesthesia 4.5 oral endotracheal tube (ETT)wassecured to the boy’s chin with plastic tape and Tegaderm dressing. We checked the ETT connections, then the patient was prepped and draped. The flow sensor alarmed low flow 10 minutes later. Tidal volume decreased. To solve the cause of low flow alarm we firstly expected the anesthesia ventilator, the connectionsof oxygen intake and the circuit of anesthesia. There was a leak in the system. We disconnect and reconnected the ETT. After reconnection, the ventilation didn’t improve. Tidal volume dropped immediately to 0 ml. We removed the surgical drapes to examine the patient. The patient was in cyanosis with no chest rise. We removed the ETT immediately, rapidly intubated again. After ventilating with 100% oxygen, oxygen saturation increased to 99%. We didn’t suspect broncospasm or laryngospasm. The patient was reprepared and surgery proceeded uneventfully. The postoperative period was unremarkable.
What we saw then the tegaderm in the ETT causing the obstruction internally in the distal end of the ETT by migration.
There are several acute management steps to consider when assessing the deterioration of oxygenation for an intubated patient. First tube occlusion must be considered. Occlusion of the endotracheal tube is very serious and life threatening event. Manuel ventilation should be the first , removing of the tube should be the second attempt in case of impossible suction. When it is not possible to remove the obstruction quickly, rapid reintubation must be performed [1,2].
There have been case reports which have been shown various tecniques in dealing with blood clot impaction in the ETT. Once obstruction is suspected, nearly all reports indicated a common algorithm for the management of the obstructed ETT. More importantly this rapidly results in life threating ventilatory problems.
In conclusion we present a patient who became hypoxic severely during the surgery due to the occlusion. Weare unaware of any similar case as ours, causing obstruction of the airway. Without any panic we overcame this serious complication which could have a fatal consequence.
Figure 1, 2, 3: Views of the endotracheal tube
References
- Hofstetter C, Scheller B, Hoegl S, Mack MG, Zwissler B, Byhahn C. Cuff overinflation and endotracheal tube obstruction: case report and experimental study. Scand J Trauma Resusc Emerg Med 2010;18(18):1-5.
- Shah DM, Sinn J. Endotracheal suction catheter as a foreign body in a neonate.J Paediatr Child Health. 2010,46:209