


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
"A Case of Anaphylaxis after Blood Transfusion" - An Alarm to the Anesthesiologist and Surgeon
Venkata Ramana Murthy V1, Jambukeshwar Kumar B2, Chandrasekhar K3, Srilakshmi T4
2.Senior Lecturer, Department of Oral and Maxillofacial Surgery, Vishnu Dental College, Bhimavaram, India
3.Professor, Department of Anesthesiology, NRI Institute of Medical Sciences, Visakhapatnam, India
4.Duty Medical Officer, Visakhapatnam, India
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Blood transfusion reactions do occur in the practice of blood transfusion which always aims at reducing unnecessary transfusions without compromising the standards of quality and safety. However, many non-hemolytic reactions like Anaphylaxis do occur in 1:20 000 to 1:50 000 of transfusions annoying the entire anesthetic team and making surgical management a herculean task. Reactions usually begin within a few seconds or minutes after the start of the transfusion. Patients can present with a sudden onset of severe hypotension, cough, bronchospasm (respiratory distress and wheezing), laryngospasm, angioedema, urticaria, nausea, abdominal cramps, vomiting, diarrhoea, shock and/or loss of consciousness. This may be a fatal reaction.
We report a case of Anaphylaxis following blood transfusion in a case of facial trauma following road traffic accident with hemorrhage, underwent open reduction and internal fixation in our hospital who has presented with classical symptoms of anaphylaxis which changed the entire course of the treatment plan which emphasizes the importance of preparedness towards any untoward complications.
blood transfusion, anaphylaxis, facial trauma, Anesthesiology
The appropriate use of blood and blood products means the transfusion of safe blood products only to treat a condition leading to significant morbidity or mortality that cannot be prevented or managed effectively by other means. Transfusion carries the risk of adverse reactions and transfusion transmissible infections. Blood should not be transfused unless it has been obtained from appropriately selected donors, has been screened for transfusion transmissible infections and tested for compatibility between the donor’s red cells and the antibodies in the patient’s plasma, in accordance with national requirements. Transfusions of whole blood, red cells or plasma are often given when other treatments, such as the infusion of normal saline or other intravenous replacement fluids would be safer, less expensive and equally effective for the treatment of acute blood loss. Patients’ transfusion requirements can often be minimized by good anesthetic and surgical management. If blood is given when it is not needed, the patient receives no benefit and is exposed to unnecessary risk of adverse reactions. Blood is an expensive, scarce resource. Unnecessary transfusions may cause a shortage of blood products for patients in real need [1].
2. Case Report
A 42 years old man reported to the department of oral and maxillofacial surgery with facial asymmetry caused by swelling on the left side of the face with history of road traffic accident with hemorrhage 4 days before. He noticed painful swelling following trauma with associated pain, limited mouth opening, difficulty in speech and swallowing. Preoperative assessment of hemoglobin was 7.8gm%, hematocrit of 30% with blood group B positive with no prior history of blood transfusion. The patient was diagnosed with mandibular angle fracture and was planned for Open reduction and internal fixation under General Anesthesia with hypovolemic shock.
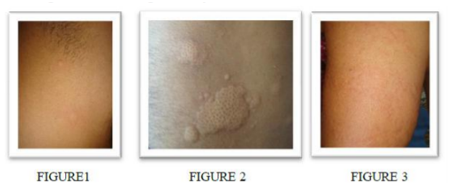
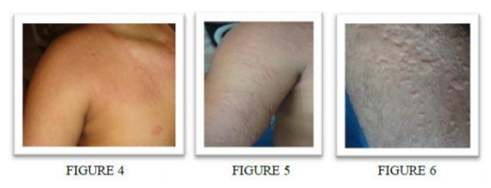
After complete evaluation the case was discussed with the anesthesiologist regarding fitness to operate under general anesthesia. As per the advice by the anesthetic team preoperative 1 unit of blood transfusion was planned. Cross matching was done, high risk consent was taken and was patient was counselled accordingly. In the ward, 4days after hospitalization prior to transfusion all the vitals were measured, pulse 82/minute, blood pressure was 110/74mm of Hg, respiratory rate was 16cycles/minute, a febrile. Initially, patient developed hypotension with blood pressure of without any signs of breathlessness, but there was fall of blood pressure to 90/60mm of Hg, increased heart rate 112/minute with characteristic rash developing on the abdomen progressing on to forearm, then on the thighs in short span increasing with breathing severity alarmed us to make a diagnosis of anaphylaxis. Upon advice from the anesthesiologist transfusion was stopped immediately and supportive, symptomatic therapy was started with oxygen, injection diphenhydramine 50 mg IV, to correct hypotension, adrenaline (subcutaneous) at 0.3ml (1:1000, dilution) were administered and observed for resolution of signs and symptoms. The patient recovered and attained normalcy after 24 hrs. The patient was monitored for any signs of delayed reactions. Surgery for Open reduction was subsequently done under local anesthesia, as patient have not given consent for general anesthesia. The main concern was anaphylactic reaction has changed the entire treatment plan. The patient was operated and was discharged uneventfully, and subsequently kept on hematinics for a period of 1 month.
3. Discussion
A transfusion reaction is said to be acute if it occurs during or within 24 hours of transfusion or delayed if it occurs beyond 24 hours up to 4 weeks after transfusion. Acute transfusion reactions (ATR) occur at a rate of 0.5–3% [2]. Allergic transfusion reactions are also common. It occurs in about 1–3% of all transfusions and is more frequent in atopic individuals [3].
Patient developed features of anaphylaxis soon after 10 minutes of blood transfusion around 7 ml of blood was transfused and patient reported the symptoms. Immediately upon advice from the anesthesiologist we stooped transfusion. Immediate evaluation to exclude other pulmonary involvement both bacterial contamination and hemolytic reactions were considered [4,5]. The practice of blood component therapy (BCT) is associated with improved utility of blood (a single whole blood unit may be separated into three different components for possible use by three different patients[5]. However prompt recognition, vigilance on blood packets and patient’s prior history of allergy can overcome severe untoward reaction. It is a type 1 hypersensitivity reactions mediated by IgE bound basophils and mast cells in previously sensitized blood recipients. When re-exposed to implicating allergens (most often plasma proteins) in the donor blood, antigen-antibody interaction causes cross-linking of bound immunoglobulins on mast cells, hence degranulation. Preformed vaso-active amines (principally histamine and serotonin) in mast cells and basophils are released [6]. As a late response, leukotrienes, slow release substances of anaphylaxis are also released. Typically, patient develops a localized or systemic urticarial rash with erythema and pruritus which was evident all the parts of the body [7]. In severe allergies or anaphylactic reactions, other organs systems such as the chest, cardiovascular and gastro-intestinal are involved which was quite evident in our case. Generally, allergies are more troublesome than dangerous.
4. Conclusion
Improved knowledge and awareness among the clinical staff to correctly recognize the complications of blood transfusion is an everyday challenge. However with prompt reaction and response to reactions like anaphylaxis safety, medico legal issues relating to blood transfusion reactions can be prevented with proper blood transfusion practices with proper counselling and high risk informed consent. It is the responsibility of entire team of anesthesiology and surgery team to prevent and recognize non –hemolytic anaphylaxis as early as possible to intervene and promote good transfusion practice enhancing overall safety.
References
- Indrikovs AJ. Accidental transfusion with ABO incompatible blood: process for analysis of the contributing causes. Sangre (Barc). 1997 June; 42(3):205-13.
- Fry JL, Arnold D, Clase C, Crowther M, Holbrook, Traore A, et al. Transfusion premedication to prevent acute transfusion reactions: A retrospective observational study to assess current practices. Transfusion. 2010; 50:1722–1730.
- Hendrickson JE, Hillyer CD. Non-infectious serious hazards of transfusion. Anesthesia and Analgesia. 2009; 108(3):759–69.
- Looney MR, Groopper MA, Mathay MA. Transfusion related acute lung injury: a review. Chest 2004; 126:249- 58. 2 Toy P, Gajic O.
- Transfusion related acute lung injury. Anesth Analg 2004; 99: 1623-24.
- World Health Organization. The clinical Use of Blood. WHO Blood Transfusion Safety Geneva; 2001.
- Pomper GJ. Febrile, allergic and nonimmune transfusion reactions. In: Simon TL, et al. (eds.). Rossi’s principles of Transfusion Medicine. West Sussex. Wiley-Blackwell. 2009; 53:826- 846.