


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Right Lung Collaps with Selective Placement of a Bifurcated Bronchial Blocker in the Tracheal Bronchus and the Right Main Bronchus
Alaleh Zamanbin1, Mohamed Bentala2, Thierry V Scohy1, Bastiaan M. Gerritse1
2.Department of Cardiothoracic surgery, Amphia Hospital, Breda, the Netherlands.
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This case report shows how a bifurcated bronchial blocker can be a safe alternative to a double lumen tube when obtaining right lung isolation in an anatomical variant. Double lumen tubes are the most used devices when one lung ventilation is required. Bifurcated bronchial blockers may have an advantage regarding safety and ease. This case report presents the use of a bifurcated bronchial blocker in a tracheal bronchus and right main bronchus, after a failed procedure with a double lumen tube.
Bifurcated bronchial blocker; Double lumen tube; One lung ventilation; Right lung isolation, Anesthesiology
A tracheal bronchus (also known as a pig bronchus) is an anatomical variant where an accessory bronchus originates directly from the supracarinal trachea. The incidence is in the range of 0, 1-2%, and mostly asymptomatic, this anatomical variant can be a challenge when obtaining right lung isolation. Subsequently will be presented how right lung isolation was obtained by a bifurcated bronchial blocker, after a previously failed procedure with a double lumen tube.
2. Case Report
A 66 year old woman (length 164 cm, weight 76 kg) was scheduled for a mini-maze procedure by endoscopic ablation using bilateral thoracoscopy. Medical history consisted of paroxysmal atrial fibrillation, hypertension and diabetes mellitus treated by oral medication.
After induction with propofol, sufentanil and rocuronium, and subsequent continuous propofol maintenance, patient was intubated with a 8 mm single-lumen endotracheal tube through which a bifurcated bronchial blocker (BB) (Rüsch EZ-Blocker, Teleflex Morrisville, NC USA) was inserted through the multiport adapter and advanced under fiberoptic control. Through fiberoptic visualisation was diagnosed that the bronchus of the right upper lobe originated partially from the trachea itself. Placement of the BB on the main carina was obtained. However, insufflation of the right side balloon only isolated the right bronchus intermedius, not the bronchus to the right upper lobe. As a bilateral thoracoscopy with complete right lung collaps could not be obtained, the consultant anesthesiologist decided to exchange the single lumen endotracheal tube for a left sided double lumen tube (DLT) (Rüsch Teleflex, Morrisville, USA). Two attempts were made to insert a DLT size 37 and 35, but neither could be advanced through the vocal cords due to size mismatch. Considering the risk of laesions to the airway, further attempts to insert a device were abandoned. After antagonizing the muscle relaxation, the infusion of propofol was discontinued and patient awoke without further incident, ventilated by bag and mask.
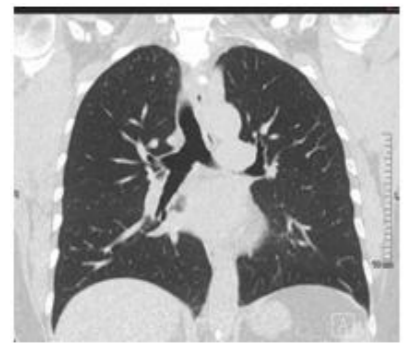
A cat scan (Figure.1) showed that the bronchus to the right upper lobe originated maximum 0.5 cm proximal of the right bronchus intermedius and partially from the trachea itself. Both patient and consultant cardiologist expressed a strong desire for the mini-maze procedure to be performed, as it was as the most effective treatment. A consultant anesthesiologist with an extensive experience with bifurcated BB (>500 procedures) was brought in on the case, and the patient was informed and rescheduled for the procedure. After induction of anesthesia with propofol, sufentanil, rocuronium and continuous infusion of propofol, a single lumen endobronchial tube size 7 was inserted. The bifurcated BB was advanced through the endotracheal tube under fiberoptic visualization, with simultaneous ventilation of the patient through the endotracheal tube. On placement of the bifurcated BB just above the main carina, the left balloon was inflated causing the bifurcated BB to veer to the right. By pushing the BB slightly downwards, the empty right balloon of the BB entered the tracheal bronchus of the right upper lobe. The left balloon was subsequently deflated, causing the empty left balloon to enter the right bronchus intermedius. By inflating both left and right balloon, the right lung could be isolated and the mini-maze on the right could be performed (Figure. 2).
To complete the ablation of the atria, the bifurcated BB had to be repositioned to the main carina to isolate the left lung. The surgery was completely performed without any events. The patient was detubated immediately following the procedure and had a uneventful recovery.
3. Discussion
A DLT is the most commonly used device in one lung ventilation. The bifurcated bronchial blocker has proven to be a safe alternative [1]. Its design makes positioning easier, and the bifurcated BB may be positioned more safely and easily than other types of bronchial blockers [2,3,4]. As this report shows, the bifurcated BB can be placed in both the right tracheal bronchus and right bronchus intermedius by contralateral balloon insufflation and gentle manipulation. By subsequent insufflation of both balloons, full right lung isolation can be obtained [5].
References
- Efficiency, Efficacy, and Safety of EZ-Blocker Compared with Left-sided Double-lumen Tube. Mourisse, et al. Anesthesiology. March 2013 - Volume 118 - Issue 3: 550–561.
- Randomized clinical trial comparing double-lumen tube and EZ-Blocker® for single-lung ventilation. Ruetzler, et al. British Journal of Anaesthesia. 2011, 106 (6): 896–902.
- Lung isolation with a new Y-shaped endobronchial blocking device, the EZ-blocker. Mungroop et al. Br J Anaesth. 2010;104:119– 20.
- Choosing a lung isolation device for thoracic surgery: a randomized trial of three bronchial blockers versus double lumen tubes. Narayanaswamy et al. Anesth Analg. 2009; 108:1097–101.
- Clinical experience with a new endobronchial blocker: the EZ-blocker. Tamas, et al. Journal of Anesthesia. June 2012, Volume 26, Issue 3: 375-380.