


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Continuum of Care of Clonazepam Misuse Prescription in Mental Health Psychiatry Outpatient Clinics: A Project from K.S.A
Dr. Eltoum, Etidal Abdelrahman
Copyright : © 2018 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Clonazepam Misuse, Prescription,Mental Health, Psychiatry Outpatient Clinics, Project from K.S.A,Addiction
1. Introduction
What is CLONAZEPAM? Is a medical prescribed drug that belongs to a group of medication called long-acting benzodiazepine drugs? (4)
Clonazepam is known also by the brand name Klonopin; it is the third of the most prescribe benzodiazepine in the USA behind Alprazolam (Xanax) and Lorazepam (Ativan) (4) These medications have very similar properties, but vary in their speed of onset and duration of their effects. Clonazepam is not recommended for the elderly because increase risk of cognitive impairment, drug accumulation, sedation and fall. (33) It is associated with a number of risks, most worrisome Person can physically dependent on the drug in a short period of time, even when using the drug as instructed.

Definition of Substance Misuse: Is harmful use of substance (like drugs and alcohol) for non-medical purposes.
The term “substance misuse” often refers to illegal drugs. However, legal substance can also be misused, such as alcohol, prescribed medication, caffeine, nicotine and volatile substances (e.g. petrol, glue, paint). (11)
Dependence: A state in which an organism function normally only in the presence of a drug. Manifested as a physical disturbance when the drug is removed (withdrawal). (66)
Addiction: Is the physical and/or psychological need for a substance, due to regular, continued use. Some substances are highly addictive, others are less addictive. However, the symptoms of addiction are similar no matter which substance is used. (11)
Withdrawal Symptoms of Clonazepam: The withdrawal effects can be dangerous. Abrupt withdrawal from Clonazepam may result in the development of the withdrawal syndrome causing psychosis, dysphoric mood, irritability, aggressiveness, anxiety, and hallucinations.
Sudden withdrawal may also induce the potentially life threatening condition- status epilepticus – in which the brain is in a state of persistent seizure. (16) Benzodiazepines such as Clonazepam in particular, should be reduced slowly and gradually before discontinuing the drug to reduce withdrawal effects. Carbamazepine (Antiepileptic) has been used in the treatment of clonazepam withdrawal and has been found to be ineffective in preventing Clonazepam withdrawal status epilepticus from occurring, which is important to take into consideration. (75)
Overview about Substance Abuse in K.S.A
Among Saudi patients in addiction treatment settings, the most commonly abused substances were amphetamine (4-70.7%), heroin (6.6-83.6%), alcohol (9-70.3%), and cannabis (1-60%).
Over the past decade, there was an increase in the use of cannabis and amphetamine and decrease in the use of heroin and volatile substances.
Peer pressure and psychosocial stresses were risk factors for initiation as well as relapse of substance abuse.
Anxiety, depression and hepatitis were the most common comorbid disorders among the Saudi patients.
Importance: -No available control medication prescription statistics.
Lack of surveillance for possible misuse.
Work overload.
Patient aggression.
2. Objectives
To collect basic data on multiple and diverse drug dependence and aggression in work place.
To apply a cost effective measure which is capable to minimize the possible misuse.
To manage control prescriptions among psychiatry patients and reduced patient aggression in psychiatry settings and reduce work overload.
Prescription Protocol:
If the patient is Dependent on BZD– referral to Detox Centre.
If the patient is Abusing BZD: Education Session – 30 min. Weekly visit to Clinic Gradual reduction of dose.
If the patient need to Continue on medication:
Prescription of minimum dose
Monthly prescription Restriction sign (NO BENZO) from ER/Pain Clinic or any other medical services.
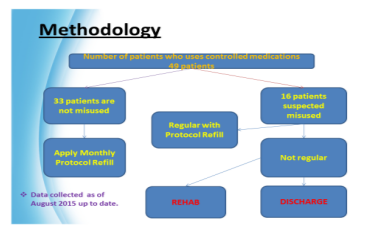
3. Methodology
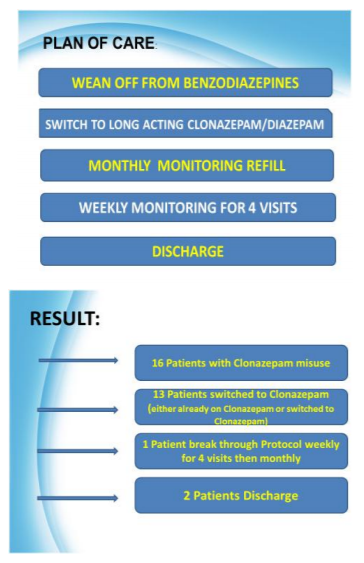
We continue our previous plan to move patient through different phases including:
1st Phase - to try wean them off from benzodiazepine.
2nd phase –switch to Clonazepam as long acting benzo
3rd phase- which is applying our strict monthly visit protocol
4th phase – which include those with break through protocol to give them a weekly refill for 4 consequent visit and then back to monthly refill and if they again break through protocol to discharge from the clinic
Inclusive criteria
All schizophrenic patients who are on antipsychotic medications
Exclusive criteria
1-Children
2-Elderly patient with Dementia
4. Discussion
Our clinic data shows that we have significant number of patients on BZD.
Clonazepam have high percentage so we concentrate our effort on those patients.
Our old way system of dealing with them is associated with low outcome for patients and risk/load to staff. Sometime patients became aggressive if prescription is not done.
Diagnosis correlated to aggressive behavior, such as: S/P Brain Surgery Cancer: more common breast cancer, osteosarcoma. Human immune virus.
5. Conclusion
Successful monitoring is need to be applied in all Psychiatry Clinics. More accurate reliable data is required. Current service needs to improve.
Future Plans
Apply the same restriction protocol to the remaining psychiatric clinics.
Enhance national epidemiology data collection system.
Raise public awareness about drug risk to addiction.
Restriction method applied on patient charts and ICIS with sign “No benzodiazepine” mainly from Emergency Department or other medical services.
Department of Emergency agreed upon to release benzo in attendance of psychiatrist.
Develop a plan to control aggression like Code White by direct or indirect measure.
Liaison with Alamal Hospital for detox patients because the government put all their financial effort in one place as big as professional Detox Centre in the Capital City of Riyadh.
References
- Gillies, Donna; Sampson, Stephanie; Beck, Alison; Rathbone, John (2013-04-30). "Benzodiazepines for psychosis-induced aggression or agitation". The Cochrane Database of Systematic Reviews. CD003079. doi:10.1002/14651858.CD003079.pub3. ISSN 1469-493X. PMID 23633309.(4)
- Authier, N.; Balayssac, D.; Sautereau, M.; Zangarelli, A.; Courty, P.; Somogyi, AA.; Vennat, B.; Llorca, PM.; Eschalier, A.
(November 2009). "Benzodiazepine dependence: focus on withdrawal syndrome". Ann Pharm Fr (6): 408–13.
doi:10.1016/ j.pharma.2009.07.001. PMID 19900604. (67) - Lander CM; Donnan GA; Bladin PF; Vajda FJ (1979). "Some aspects of the clinical use of clonazepam in refractory epilepsy". Clin Exp Neurol. 325–32. PMID 121707.(16)
www.lifeline.org.au/static/uploads/files/what-is-substance-misuse-and-addiction-wfyzigyyljub .pdf(11) - National Institute on Drug Abuse. (2003). Preventing Drug Use among Children and Adolescents: A Research-Based Guide for Parents, Educators, and Community Leader(66)
https://www.mayoclinic.org/drugs-supplements/clonazepam-oral-route/before-using/drg-20072102(33)