


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Antibiotic Resistance Pattern of Moraxella Catarrhalis in Patients with Respiratory Tract Infections at Tamale Teaching Hospital
Dr.Abdallah Iddrisu Yahaya1*, Doklah Kwame Anthony2
2.Catholic University College of Ghana and Editor in Chief, Todayingh News
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
The large majority of antibiotics currently used for treating infections and the antibiotic resistance genes acquired by human pathogens each have an environmental origin. Recent work indicates that the function of these elements in their environmental reservoirs may be very distinct from the “weapon-shield” role they play in clinical settings. Changes in natural ecosystems, including the release of large amounts of antimicrobials, might alter the population dynamics of microorganisms, including selection of resistance, with consequences for human health that are difficult to predict.
Both antibiotic biosynthetic genes and resistance-conferring genes have been known to evolve many years ago, long before clinical use of antibiotics. Hence it appears that antibiotics and antibiotics resistance determinants have some other roles in nature, which often elude our attention because of overemphasis on the therapeutic importance of antibiotics and the crisis imposed by the antibiotic resistance in pathogens. In the natural milieu, antibiotics are often found to be present in sub-inhibitory concentrations acting as signaling molecules supporting the process of quorum sensing and biofilm formation. They also play an important role in the production of virulence factors and influence host–parasite interactions (e.g., phagocytosis, adherence to the target cell, and so on). The evolutionary and ecological aspects of antibiotics and antibiotic resistance in the naturally occurring microbial community are little understood.
ESBLS, Tamale Teaching Hospital, Chest Clinic, Multiple drug resitance, Antobioic susceptibility,Public Health and Community Medicine
1. Introduction
The rapid emergence of resistant bacteria is occurring worldwide, endangering the efficacy of antibiotics, which have transformed medicine and saved millions of lives. Many decades after the first patients were treated with antibiotics, bacterial infections have again become a threat. The antibiotic resistance crisis has been attributed to the overuse and misuse of these medications, as well as a lack of new drug development by the pharmaceutical industry due to reduced economic incentives and challenging regulatory requirements. The Centers for Disease Control and Prevention (CDC) has classified a number of bacteria as presenting urgent, serious, and concerning threats, many of which are already responsible for placing a substantial clinical and financial burden on the U.S. health care system, patients, and their families. Coordinated efforts to implement new policies, renew research efforts, and pursue steps to manage the crisis are greatly needed.
The term “antibiotics” was first coined by the American microbiologist Selman Waksman and his colleagues to describe chemical substances produced by microorganisms and having antagonistic effects on the growth of other microorganisms. It excluded synthetic antimicrobials (sulfur drugs) and biological products of non-microbial origin having antagonistic effects on bacteria. Though antibiotics were introduced into the clinical practice only in the middle of the last century, the use of microorganisms for the management of microbial infections in ancient Egypt, Greece, China, and some other places of the world is well-documented. The modern era of antibiotics started with the serendipitous discovery of penicillin from the culture filtrate of a fungus, Penicillium notatum by Alexander Fleming in 1928 (Fleming, 1929).
In the present scenario, antibiotics available in the market are either produced by microbial fermentation or are derived via semi-synthetic route using the existing antibiotic backbone structure. They are classified into different chemically defined groups. Antibiotics target bacterial physiology and biochemistry, causing microbial cell death or the cessation of growth. A significant number of these antibiotics affect cell walls or membranes (e.g., β-lactam and glycopeptides), while several others exert their antibacterial activity by targeting protein synthetic machinery via interaction with ribosomal subunits and these include antibiotics such as macrolides, chloramphenicol, tetracycline, linezolid, and aminoglycosides. Other “mechanistic” groups include molecules which interfere with the nucleic acid synthesis [e.g., fluoroquinolones (FQ) and rifampin], while some others exert their effects by interfering with the metabolic pathways (e.g., sulphonamides and folic acid analog) or by disruption of the bacterial membrane structure (e.g., polymyxins, daptomycin, and others).
A surge of discovery of several such antibacterial and antifungal antibiotics accompanied with a new generation of semi-synthetic drugs initially led to euphoria that any infectious disease could be successfully controlled using antibiotics. However, emergence and propagation of bacterial strains, resistant to almost all the therapeutically useful antibiotics during the past few decades revealed the limitation of the wonder drugs. Though imprudent and excessive use of antibiotics is highlighted as a major causative factor behind the setback, it is evident by this time that antibiotic resistance does not call for exposure of the organisms to antibiotics. It is also found that genes involved in the biosynthesis of antibiotics and antibiotic resistance evolved thousands of years before antibiotics were introduced into the clinical practice. Hence both antibiotic and its resistance determinants have some other role in bacterial physiology.
2. Background
The emergence and spread of antibiotic resistant strains particularly the detection of the Extended Spectrum Beta-lactamases (ESBLs) Salmonella species, is fast becoming an emerging world threat. ESBLs frequently occur in K. pneumonia but recent studies have increasingly reported its occurrence in the Salmonella specie and other gram-negative organisms. Such Salmonella strains pose significant health problems worldwide by virtue of their acquisition of resistance against most beta-lactam antibiotics, which were previously used for treatment of Salmonella infections.
ESBLs are enzymes capable of hydrolyzing penicillin, cephalosporin and oxyiminino-β-lactam compounds (i.e. cefuroxime, third generation cephalosporin and aztreonam) with cephamycins and carbapenems as exceptions. Most ESBLs belong to the Ambler class “A” β-lactamases and are inhibited by β-lactamase inhibitors (clavulanate, sulbactam and tazobactam). ESBLs are plasmid-mediated and as a result, are easily transmitted among members of the Enterobacteriaceae family.
This potential exacerbates the spread of resistance against β lactams and other commonly used antibiotics including quinolones and aminoglycosides. This has further limited the therapeutic options available and hence complicated the treatment and management of infections by such organism.
The determination of antibiotic susceptibility pattern and multidrug resistant pattern of infectious organisms is therefore necessary to provide a vivid guide for physicians to make informed drug choices during the management and treatment of patients. It is also important in ensuring the effective and quick treatment of Salmonella infections as well as other infections without aggravating the illness. This minimizes antibiotic resistance and cost of treatment.
The study was conducted in Tamale teaching Hospital.
Sputum specimens were collected from patients with lower respiratory tractinfections.
Specimens were screened based on Bartlett’s grading of sputum Gram stain (Koneman’s Color Atlas and Textbook of Diagnostic Microbiology, 6th edn).
The Ministry of Health of Ghana in 1983 published a list of Essential Drugs with Therapeutic Guidelines to aid the rational use of drugs. The Government of Ghana, through the National Drug Policy remains committed to ensuring the availability and accessibility of good quality medicines for all people, and that these medicines are affordable and are rationally used The Standard Treatment Guidelines have been prepared to assist and guide prescribers, pharmacists, dispensers and other healthcare staff in providing quality care to patients.
Based on these facts it has become increasingly necessary to conduct this study at the Tamale Teaching Hospital in order to monitor antibiotic usage and this would serve as a baseline for detection of significant changes in prescription patterns and act as a guideline for antibiotic education program. There is a dearth of data on not only the Resistance producing ESBL specie but also their multi drug resistance pattern amongst human subjects. The aim of this study was therefore to evaluate the prevalence of Resistance producing ESBLs strains by phenotypic methods and their profile of drug resistance amongst patients with respiratory tractinfections in Tamale Teaching Hospital of Northern Ghana.
The protocol for this study was approved by the Ethical Committees of the Tamale Teaching Hospital (TTH). Approval was also obtained from the Ministry of Health. Informedconsent was sort from all study participants.
3. Literature Review
Antibiotics are one of the most common drugs prescribed in hospitals today. It has been estimated that up to a third of all patients receive at least one antibiotic during hospitalization. According to the ministry of Health, the cost involved is therefore correspondingly high and up to 40% of a hospital‘s drug expenditure may be devoted to the purchase of antibiotics (WHO, 2016).
In the past decade, there has been an alarming trend towards increase antimicrobial resistance in many human pathogens around the world. Of the many possible factors responsible for these developments, the overuse and inappropriate prescribing of broad spectrum antibiotics has been Implicated.
The in-hospital use of antibiotic drugs has been a major concern in the last few decades for several reasons. For the purchasers of health care services and administrators, antibiotic drugs account for a major proportion of the escalating drug budget, especially in hospitals. The overuse and misuse of antibiotic drugs is considered to be one of the reasons for increasing resistance among various pathogens. These worries have led to the implementation of strict antibiotic policies in hospitals in many countries, with different strategies and different outcomes. Monitoring of drug use is essential in order to follow the effects of, and adherence to, the hospital‘s antibiotic policies. Patient medical records may be reviewed for this purpose, but this method can be quite exhaustive.
The ultimate goal of drug utilization research must be to assess whether drug therapy is rational or not. The principal aim of drug utilization research is to facilitate the rational use of drugs in populations. For the individual patient, the rational use of a drug implies the prescription of a well documented drug at an optimal dose, together with the correct information, at an affordable price. The observed patterns of drug use can be compared with the current recommendations and guidelines for the treatment of a certain disease.
There have been numerous studies on patterns of antibiotic usage in hospitals. Many of these studies were however conducted in developed countries. Data from developing countries are scarce.
Antimicrobial use should be monitored in terms of the type and degree of irrational use and several well-established methods exist. Aggregate antimicrobial drug consumption data can be used to identify the most expensive and highly used antimicrobials, or to compare actual consumption with expected consumption (from morbidity data). Anatomical Therapeutic Classification (ATC) / Defined Daily Dose (DDD) methodology can be used to compare antimicrobial consumption across institutions, regions and countries. Indicators can be used to investigate antimicrobial use in primary health care.
Focused antimicrobial use evaluation (drug utilization review) can identify problems concerning the use of specific antimicrobials or the treatment of specific infections, particularly in hospitals.
In view of increasing antibiotic resistance as well as the escalating cost of antibiotic therapy, the Ministry of Health of Malaysia embarked on a project to assess antibiotic usage in its hospitals in 1989. The main objectives of this study were to (i) ascertain pattern of use of antibiotics, (ii) identify deficiencies and implement remedial measures, and (iii) evaluate the effectiveness of these remedial measures. This was a prospective, descriptive and cross-sectional survey of antibiotic prescriptions issued for inpatients at six general hospitals situated in various parts of the country. The sampling unit was an antibiotic prescription regardless of whether the prescription issued was for a single agent or a combination of antibiotics. The doctors in the study hospitals were aware of the survey that was being carried out. This by itself would have influenced the prescribing practices of the doctors. Despite this, the lack of compliance with issued guidelines was very evident [1].
A survey by the Intercontinental Medical Statistics Pharma Strategy Group (IMS HEALTH) of antibiotic usage in hospitals in France, Germany, Italy, Spain, and the United Kingdom has illustrated the diversity between countries, the implications for antibiotic resistance, and how difficult it would be to have a European Union policy on prescribing antibiotics in hospital to prevent the emergence of resistant organisms. The survey was part of a regular audit of antibiotic treatment in hospital in 18 countries. Data on antibiotic use showed that in Italy and Spain the number of days of antibiotic treatment had declined between 1995 and 1997 whereas they have increased in France, Germany, and the UK. The use of combination treatment has increased over the same period in the UK compared with Germany, Italy, and Spain where its use has declined.
The Finnish Hospital Infection Program (SIRO) conducted the first national prevalence survey of nosocomial infections (NIs) in 30 Finnish acute care hospitals during February–March 2005. The objective was to analyze the amount and type of antimicrobials administered in acute care hospitals based on data collected in this national survey. All inpatients present on the study day in acute care wards for adults were examined (n=8234). Infection control practitioners, who attended a 1-day training course organized by SIRO, collected data with link nurses and ward staff. Data on antimicrobials were recorded on the study day and retrospectively for the previous 6 days (a 7-day window), allowing for estimation of use-density among the study population. No data on dose, timing or dosing interval of antimicrobials or on antimicrobials administered as surgical prophylaxis in operating theatres were recorded. The study provided an overview of antimicrobial use in Finnish acute care hospitals. The prevalence of antimicrobial use was high; more than one-third of patients had received an antimicrobial or antibacterial on the study day. In previous studies with a similar study design, from 16% (Denmark), 18% (Germany), 28% (Scotland) to 40% (USA) of hospital patients were given antibacterial. NIs contributed markedly to the usage in the study.
In 2004, the Ministry of Health in China published the Guidelines for Antibiotics Clinical Use and Provisions for Prescription Management as part of a national effort to improve the rational use of antibiotics and the containment of antimicrobial resistance. A pilot study was initiated in December 2004 to monitor the clinical use of antibiotics in hospitals. A baseline assessment using a retrospective survey was also conducted in December 2004. The objectives of the pilot project include: to monitor the antibiotics clinical use alongside with the antimicrobial resistance, to disseminate the information of antibiotics usage and the antimicrobial resistance, to provide analysis on the pattern of antibiotics usage and antimicrobial resistance and to develop appropriate measures for containment, and to provide evidence for revising the Guidelines for Antibiotics Clinical Use. In each hospital, the Pharmacy Department is responsible for the monitoring or collecting data on utilization and the Department of Microbiology is responsible for monitoring data on antimicrobial resistance.
To understand the situation of antibiotic usage in primary care units in Taiwan, all prescriptions were collected over a 1-week period during March 2 to March 7, 1992, December 2 to December 7, 1992, and January 14 to January 19, 1994 from out-patient clinics of public health stations located in various parts of Taiwan. In addition to all medications prescribed, information regarding patient age, sex and diagnosis were also collected. The proportion of antibiotics prescribed in total patient-visits, in patients of various age groups, in patients with various diagnoses, and the kinds of antibiotics prescribed were analyzed. Since there was no guideline for antibiotic prescription for physicians in the primary care units in Taiwan except some regulations from the medical insurance that restrict some antibiotics as second line drugs for treatment of infections, it is not surprising to find that antibiotic usage was very common and often inappropriate.
Costs and use of antimicrobial agents in 1976 at 19 hospitals were surveyed by review of pharmacy records. Total costs of antimicrobial drugs at individual hospitals ranged from $0.65 to $1.75 per patient day and accounted for 16% to 41% of total pharmacy drug costs. There was marked variation among hospitals in use of specific antimicrobial agents, especially cephalosporins and clindamycin. The cephalosporin and aminoglycoside antibiotics accounted for 66% of the total cost of antimicrobial agents. An 18-month antimicrobial drug control program at one hospital decreased antimicrobial drug costs by 31%. The major effect was in reducing cephalosporin use. The results of the control program document that a significant portion of hospital antimicrobial use is inappropriate and can be eliminated without apparent detriment to patient care.
Drug-use indicators were measured in a secondary health care facility in Lagos, Nigeria. The study was conducted in the year 2000 at the Ikeja General Hospital, Lagos, Nigeria. Drug use indicators are a set of standardized indices used to measure drug use in outpatient facilities. They provide a measure of the optimal use of these resources and can help in correcting deviations from expected standards and in planning.
Retrospective prescribing data was used and patient records were selected using a systematic sampling method. Standardized methods of investigating drug use indicators were employed in the conduct of the study. These methods recommend a study of 100 patient records in a single health facility or 30 records in 10 different clinics/ health facilities. The study was planned to investigate 600 patient records to increase the precision of the parameters. The records studied were for patients attended to at the outpatient department of the hospital in the first three months of the year 2000.
Drug use indicators include average number of drugs per patient encounter, percentage of patient encounters with a prescribed injection, percentage of patient encounters with a prescribed antibiotic to mention a few. Drug use indicators in Nigeria show very high levels and often reflect irrational drug use. The average numbers of drugs prescribed per patient had been found to vary from 3 to 7, the prescribing rate of injection has a range of 40-70% and antibiotic use rate exceeds 50%. Antibiotics were prescribed for many conditions they were not indicated for and to treat presumed infections especially cough and fevers that could not be diagnosed sufficiently on clinical grounds. This high rate of antibiotic prescribing at this hospital has been documented and has a number of implications. Firstly, newer and more expensive antibiotics are frequently prescribed which may be unaffordable to most patients and poor compliance in those who may be able to start a course but are unable to finish.
High levels of antibiotics use, often clinically unnecessary, have led to a steady increase in drug resistance. Research programmes alone are unlikely to improve antibiotic use, and findings should guide the development of priority programme activities, which include a carefully designed mix of activities by governments, health delivery systems, health training institutions, professional societies, pharmaceutical companies, consumer organisations, and international organisations. Strategies that lean too heavily on professional education are unlikely to result in large-scale or long-lasting improvement.
Patient demand is often believed to influence doctors' prescribing decisions. Various studies document physicians‘opinions that they fear losing patients if they do not provide what patients desired. Access to quality laboratory services is often seen as pivotal to the correct use of antimicrobials. Also, lack of laboratory facilities (or patients‘inability to pay for lab services), have been blamed for over prescribing of antimicrobials. Interestingly, some studies show that when laboratory facilities are available, their use is not necessarily higher. Antibiotics are often believed to have the ability to prevent disease. For example, in the Philippines, antibiotics are commonly taken to prevent diarrhea especially after eating foods of doubtful hygienic status. Studies in Zimbabwe and in the Philippines found that STDs are believed to be preventable by taking an antibiotic immediately after visiting a prostitute.
4. Methodology
1. Mixed method (qualitative and quantitative approach) of Research was used for the study
2. Clinical data from the hospital have also been gathered from various clinicians to aid with the research.
3. Laboratory data was also gathered from the Tamale Teaching Hospital to also help with the research.
4. Review of patients ‘folders, Assess drug availability from pharmacy records, Informal interviews of prescribers, scrutiny of laboratory records and observations at pharmacy.
Specimens were inoculated on blood agar and MacConkey agar. The isolates were identified by colony characteristics and biochemical tests such as catalase test, oxidase test, sugar fermentation test, DNase test, nitrate reduction test and Hugh Leifson’s oxidative and fermentative test. Moraxella catarrhalis was identified as gram-negative diplococcus on Gram’s stain. It gave positive reaction with catalase and oxidase test. Nitrates were reduced and DNase test was positive. Sugars were not fermented and Hugh Leifson’s test showed asaccharolytic type of reaction. Antibiotic susceptibility test was done by Kirby Bauer disk diffusion technique (CLSI Document, 2014). Association with demographic factors such as age, sex and various risk factors was studied.
5. Results And Discussion
To improve successful TB treatment outcomes among any population, it is important to qualitatively explore and become familiar with the background characteristics of the TB patients and factors associated with unsuccessful treatment outcomes so as to develop specific strategies for successful treatment outcomes since one intervention might not be suitable for all cases considering the huge diversity of the background characteristics of TB patients.
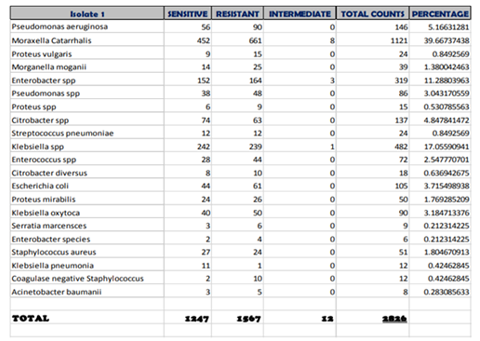
From the analysis of our results as reported at the TTH micro biology laboratory, 2862 samples were taken of which Total number of cases (Isolates) resistance to the Various Antibiotics is 1567.
Total number of cases (Isolates) sensitive to the Various Antibiotics is 1247.
Total number of cases (Isolates) Intermediate to the Various Antibiotics is 12.
This is comparable to work done by KomfuAnokye and Korle-bu in august 2013. They found that, almost all antibiotics were resistant to the microbs they tested against. this included, tetracycline, cotrimoxazole, Ampicillin, chloramphenicol and Penicillin were all more than 80 percent in resistance to the bacteria tested.
For the second generation cyclosporin’s antibiotic tested such as flucloxacillin, cefuroxime, cefotaxime and ceftriaxone were also moderately resistant (above 20 percent in resistance.)
Compared to our findings in the micro biology department of TTH, Amikacin, kanamycin, Gentamicin and chloramphenicol were still found to be potent against the microbs tested. Isolations analyzed showed that Moraxella Catarrhalis was the most prevalent in TTH respiratory patients with the frequency of 1121 representing 40 percent of the resistant species.
On several analysis, Moraxella Catarrhalis is only susceptible to gentamicin, amikacin, chloramphenicol, ciprofloxacin. Whereas all other antibiotics were found to be resistant. Klebsiella, Citrobacter and Morganella morganii, Citrobacter diversus, Citrobacter spp were also found to follow the same trends:
susceptible to gentamicin, amikacin, chloramphenicol, ciprofloxacin. In TTH, mostly, antibiotics is started without being completed, this trends start from accident ad emergency wards, continuous at opd, same at male, female wards pediatric and O and G.. when antibiotics is started, microbs which are not totally destroyed but survived will develop genoms which are to propel them with beta lactamase against lactem cyclosporin’s. This explains why the epidemic of Antibitic resistance keep emerging at TTH.
Research at the university of kalabar in Nigeria in mrch 2017, comfirmed presumptive salmonella isolates in a research paper entitled epidemic of antibiotic resistant infections: call to action for medical community from the infection disease society of America, clinical infection disease. They used comfirmatory disc method to comfirm ESBL phenotype. They found that, salmonella isolates recovered from 44 stules samples had 17.2 percent with ESBL producing strains. These were tested against third generation cephalosporins and found to be resistant against 7 of the 8-antibiotic used in that study. 77.3 percent resistants were found against ceftazidme, 59.1 percent against cefotaxime while all 44 (100 percent) salmonella strains were resistant against ceftriaxone.
In their conclusion, they wrote that, the presence of ESBL salmonella amongst isolated strains should not be over looked. They recommended continuous surveillance of antimicrobial agents and their rational use.
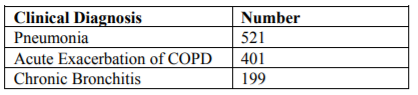
ESBL are enzymes capable of hydrolyzing penicillin, cephalosporin and oxyimino lactam compounds. ESBLs are plasmid- mediated and as a result, are easily transmitted among members of the Enterobacteriaceae family. The clinical diagnoses of the patients from whom Moraxella catarrhalis were isolated were pneumonia, acute exacerbation of COPD and chronic bronchitis. Most of the patients had expectoration of purulent sputum with low grade fever as the chief complaints.
The patients had various risk factors associated with them such as smoking, alcoholism and diabetes mellitus. The rate of isolation of Moraxella catarrhalis in patients with lower respiratory tract infections was 9.12%. This finding is similar to that of a study done by Anita KB et al., 2011 whose rate of isolation was 9.8%.
Maximum isolates were found above the age of 50years which finding is similar to that in the study by Anita KB et al., 2011. The age group distribution is also similar to a review by Catlin B Wesley, 1990. In older age group, along with decreased immunity, higher incidence of diseases such as diabetes may play a role in higher incidence of Moraxella infection in that age group. Pneumonia was the commonest presentation in the study followed by acute exacerbation of COPD and bronchitis. This finding is similar to that of HV Prashanth et al., 2011 wherein pneumonia was the commonest presentation (56.36%) followed by bronchitis (18.10%). Bronchopneumonia was also the most common presentation in the study of SB Siddeshet al., 2011.
All the cases were associated with risk factors such as old age, smoking, alcoholism and diabetes mellitus. This is similar to that of the study done by Tamang MD et al., 2005. Smoking was found to be the most common risk factor in patients with lower respiratory tract infections by Moraxella catarrhalis in our study. Smoking was also the most common risk factor in a study done by Chin et al., 1993.
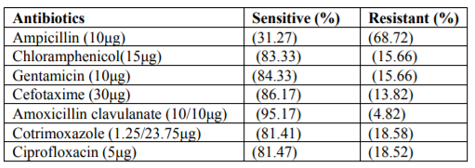
Thus in this study Moraxella catarrhalis was isolated mostly in elderly males with various risk factors. Most isolates in our study were resistant to Ampicillin (10μg) and sensitive to Amoxicillin-clavunate (10/10μg). This is a similar finding in the study of Safia Bader Uddin Shaikh et al., 2015.
The susceptibility patterns for Ciprofloxacin (5μg) and Cefotaxime (30μg) is similar to that in the study of Gupta N et al., 2011. Overall the antibiotic susceptibility pattern is consistent with the study done by Gary V Doernet al., 1996. The resistance pattern may be due to use of higher antibiotics in hospital setup.
The findings of the present study show that M. catarrhalis isolation from sputum specimen in cases of lower respiratory tract infections, especially in elderly males and in presence of risk factors, should be considered. The emergence of drug resistance especially to beta-lactam antibiotics should be borne in mind.
The conclusion to this research is that Catarrhalis is the most prevalent bacteria in tamale teaching hospital.
References
- Appel LJ, Obarzanet E, Vollmer WM,Svetkey LP, Sacks FM, et al, A clinical trial of the effects dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997; 336: 1117-1124.
- Beaglehole R. Global cardiovascular disease prevention: time to get serious. Lancet.2001; 358:661663.
- Bonita R. WR, Douglas K. The WHO STEP wise approach to NCD risk factor surveillance.
- Cordrecht: Kluwer, 2001.
- Brown MJ. Hypertension and ethnic group. Bmj.2006; 332:833-836.
- Burket BA. Blood pressure survey in two communities in the Volta region, Ghana, West Africa. Ethn Dis. 2006; 16:292-294.
- Cappuccino FP, Kerry SM, Micah FB, Plange-Rhule J, Eastwood JB. A community programme to reduce salt intake and blood pressure in Ghana BMC Public Health. 2006; 6:13.
- Cappuccio FP, Micah FB, Emmett L, Kerry SM, AntwiS, Martin-Peprah R, et al. Prevalence, detection, management, and control of hypertension in Ashanti, West Africa. Hypertension 2004; 43:1017-1022.
- Chobanian AV, Control of hypertension an important national priority. N Engl J Med.
- 2001; 345:534-535.
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr., et al.
- The seventh Report of the joint national committee on prevention, detection, evaluation and treatment of High Blood Pressure.
- Duda RB, Kim MP, Darko R, Adanu RM, Seffah J, AnarfiJK, et al. Results of the Women’s Health.
- Study of Accra: assessment of blood pressure in urban women. Int JCardiol. 2007; 117:115-122.