


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
ARC Journal of Dermatology
Volume-2 Issue-3, 2016, Page No: 3-4
Mondor’ Disease in a Patient with Hepatitis C: A Case Report
Rosa Giménez-Garcia 1,2
1.Clinical Assistant, Hospital Rio Hortega, Valladolid, Spain
2.Associate Professor, Department of Medicine, Dermatology and Toxicology, Faculty of Medicine, Valladolid, Spain.
2.Associate Professor, Department of Medicine, Dermatology and Toxicology, Faculty of Medicine, Valladolid, Spain.
Citation : Garcia RG. Mondor’ Disease in a Patient with Hepatitis C: A Case Report. ARC Journal of Dermatology. 2016;1(3):3–4.
Copyright : © 2016 Garcia RG. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1.Introduction
Mondor´disease was originally reported by Henry Mondor in 1939 as unilateral thrombosis of the superficial veins of the antero-lateral thoracic wall [1-5]. Penile Mondor´s disease is a thrombosis of the dorsal superficial veins of the penis [6] The aetiology is unknown. It is rarely associated with viral infections [7, 8] and to our knowledge the case in this report is the second case of MD in a patient with hepatitis C.
2.Case Report
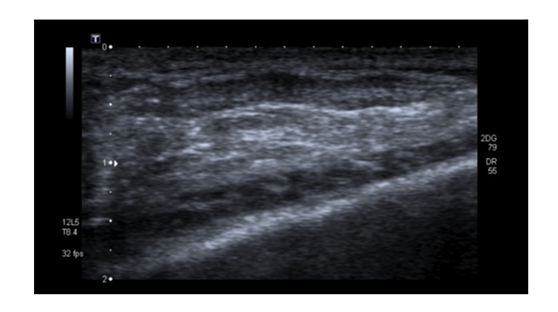
A 47-year-old woman presented to us with palpable and painful cord-like in duration on her left breast. Few days later she developed a similar lesion affecting her left thoracoepigastric vein (Figure 1). She was smoker and has a family history ok stroke but there was no history of trauma or malignancies. Bilateral mammographic examination was normal. Ultrasonographic examination showed a hypoechoic tubular structure (Figure 2) Laboratory investigations including a thrombophilia study and anticardiolipin antibodies were within normal range. Liver test revealed a light elevation of transaminases levels. Hepatitis C antibodies were positive. The patient was diagnosed as having Mondor`s disease on the basis of these findings and after 5 months of treatment with pentoxiphilline 600 twice, lesions have partially regressed.
Figure1. palpable and painful cord-like in duration on her left breast

Figure2.A tubular hypoechoic lesion is seen in the subcutaneous layer
3.Discussion
Mondor´s disease (MD) is a rare form of superficial thrombophlebitis commonly affecting the thoracoepigastric, lateral thoracic or superior epigastric veins. The pathogenesis of the disease is unclear but related with vessel-wall damage, stasis and hypercoagulable state. Histopathological findings include obstructed or obliterated vasculitis [1, 5].
Clinically is characterized by subcutaneous tender, usually unilateral cord-like phlebitis commonly on the breast or anterior chest wall but it can also involve the penis, groin, antecubital fosse, and posterior cervical region. Most of the cases are idiopathic but trauma, surgery, excessive physical activity and rarely breast carcinoma have been considered a predisposing factor. It is rarely associated with hereditary protein C, protein S deficiency or infections as herpes zoster and hepatitis C [1,7-12]. A higher prevalence of hepatitis C virus in patients with thrombosis and association with antiphospholipid antibodies has been demonstrated [10,11]. MD has been described after a mammotome biopsy and after transaxillary breast augmentation [12,13]. Doppler ultrasound is the technique of choice for confirming the diagnosis [14].
Treatment is based on nonsteroidal anti-inflammatory medication. The use of anticoagulation is controversial but may prove useful in patients with coagulation disorders.[1-5, 11]
References
- Basavaraj, K. H., N. M. Ashok, R. Rashmi, and T. K. Praveen. 2010. The role of drugs in the induction and/or exacerbation of psoriasis. Int. J. Dermatol. 49: 1351-1361.
- Allan, S. J., G. M. Kavanagh, R. M. Herd, and J. A. Savin. 2004. The effect of inositol supplements on the psoriasis of patients taking lithium: a randomized, placebo-controlled trial. Br. J. Dermatol. 150: 966-969.
- Carter, T. N. 1972. The relationship of lithium carbonate to psoriasis. Psychosomatics 13: 325-327.
- Bakker, J. B. and L. Pepplinkhuizen. 1976. More about the relationship of lithium to psoriasis. Psychosomatics 17: 143-146.
- Lowes, M. A., C. B. Russell, D. A. Martin, J. E. Towne, and J. G. Krueger. 2013. The IL-23/T17 pathogenic axis in psoriasis is amplified by keratinocyte responses. Trends Immunol. 34: 174-181.
- Petersein, C., U. Sack, R. Mergl, J. Schonherr, F. M. Schmidt, N. Lichtblau, K. C. Kirkby, K. Bauer, and H. Himmerich. 2015. Impact of lithium alone and in combination with antidepressants on cytokine production in vitro. J. Neural Transm. (Vienna) 122: 109-122.
- Hampton, P. J., R. Jans, R. J. Flockhart, G. Parker, and N. J. Reynolds. 2012. Lithium regulates keratinocyte proliferation via glycogen synthase kinase 3 and NFAT2 (nuclear factor of activated T cells 2). J. Cell. Physiol. 227: 1529-1537.
- Dowlatshahi, E. A., M. Wakkee, L. R. Arends, and T. Nijsten. 2014. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: a systematic review and meta-analysis. J. Invest. Dermatol. 134: 1542-1551.